Peer CHROs in behavioral health are treating safety investment as a labor relations strategy, and the gap between early movers and those still waiting is showing up in measurable workforce outcomes.
The organizations with stable labor relations share a pattern: they invested in safety before the grievance forced it, and they can prove what changed.
Most organizations stall because they’re waiting for union pressure to justify the spend, which guarantees they negotiate from a reactive position.
The question behavioral health CHROs keep asking each other is simple: what are other organizations actually doing about workplace violence and union safety pressure? Not what they’re planning. Not what they’re evaluating. What they’ve done, and what happened after.
The answer is splitting the field. Some peer organizations have already invested and are documenting results. Others are still waiting, and the gap between the two groups is getting harder to close.
Where Peer CHROs Are Moving
Across behavioral health, CHROs are starting to treat safety investment as a workforce stability tool tied directly to labor relations, not as a security line item managed by operations.
The shift is driven by what unions are bringing to the table. Nearly half of nurses say their employers ignore reported violence [1]. Psychiatric and substance abuse hospitals see the highest violence rates in healthcare [2]. These aren’t new numbers, but they’re now showing up in grievance filings and bargaining proposals with increasing frequency.
Peer CHROs who’ve moved on this describe a common realization: waiting for the grievance to justify the investment means you’re always one step behind the conversation. The organizations documenting the strongest labor relations outcomes are the ones that invested before the demand arrived.
What Top-Performing Organizations Do Differently
Four patterns separate the organizations with stable labor dynamics from those still managing escalating safety grievances.
They invested before the ask. The strongest peer outcomes come from organizations where safety investment preceded formal union demands. In one multi-site deployment, staff who said they’d consider leaving over safety dropped from 22% to 7% [3]. That shift happened because the investment was visible before the grievance was filed, not after.
They measure what staff feel, not just what happens. Leading organizations track safety perception alongside incident counts. Staff sentiment scores went up by as much as 38 points after investment [3]. Unions care about what their members experience, not what the dashboard says. Organizations that track perception have evidence unions accept.
They share the data openly. Peer CHROs who gave union representatives access to adoption rates, sentiment trends, and outcome metrics turned potential adversaries into advocates. Transparency converted resistance into partnership at multiple documented sites.
They frame safety as retention, not security. Organizations that positioned safety investment under workforce stabilization got CFO and CEO support faster than those who kept it in the operations budget. Workers’ comp claims dropping 24% to 50% [3] speaks the CFO’s language without translation.
The Gap Between Leaders and Laggards
The performance difference between organizations that invested proactively and those still evaluating is measurable.
Dimension
Early Movers
Still Waiting
Staff intent-to-leave over safety
Dropped to single digits
Remains above 20%
Safety sentiment trajectory
Measurable improvement documented
No baseline to compare against
Union conversation tone
Collaborative, focused on expanding what works
Adversarial, centered on what hasn’t been done
Workers’ comp trend
Declining claims, improving mod rates
Flat or rising
Board visibility
Safety metrics in workforce reporting
Safety buried in operations reports
The gap isn’t just about outcomes. It’s about positioning. Organizations with documented investment enter every labor conversation with evidence. Organizations without it enter with explanations.
“Organizations with documented investment enter every labor conversation with evidence. Organizations without it enter with explanations.”
Where Most Organizations Get Stuck
The most common stalling point isn’t disagreement about whether safety matters. Every behavioral health CHRO knows it does. The stall happens in the space between knowing and acting.
Waiting for the “right” trigger. Many CHROs wait for a serious incident or a formal grievance to justify the budget request. But by the time the trigger arrives, the investment reads as reactive. The organizations with the strongest outcomes invested before external pressure forced it.
Treating it as a security decision. When safety investment stays in the security budget, the CHRO doesn’t own it. And if the CHRO doesn’t own it, the workforce data that makes the case never gets attached. The organizations that moved fastest put it in the HR budget from the start.
Underestimating how fast peers are moving. CHROs who assume they have time to evaluate are often surprised by how far ahead peer organizations already are. The gap compounds: early movers document results, which strengthens their position, which widens the distance from organizations still in evaluation mode.
If your organization is still in the evaluation column, a conversation about what peers are seeing might help clarify the path.
If you’re reading this and recognizing your organization in the “still waiting” column, here’s what peer CHROs recommend as the first step.
Check your own data against three signals:
Exit interview themes. Are departing staff citing safety? If safety shows up in more than 10% of exits, the retention case is already there.
Grievance trajectory. Are safety-related complaints increasing, even slightly? A rising trend means union representatives are building a record.
Engagement survey gaps. Do your safety perception scores lag behind other categories? That gap is exactly what organizers use to frame leadership as disconnected.
If any of those signals are present, the peer data says the same thing: the cost of waiting is higher than the cost of acting. And the organizations that acted first are the ones sitting across the bargaining table with evidence instead of explanations.
PEER BENCHMARKS
See Where Your Organization Stands
Peer CHROs are documenting workforce outcomes from proactive safety investment. Find out how your organization compares.
Safety systems that depend on facility power or Wi-Fi fail precisely when violence risk peaks—during storms, infrastructure failures, and high-census events that strain both staff and systems.
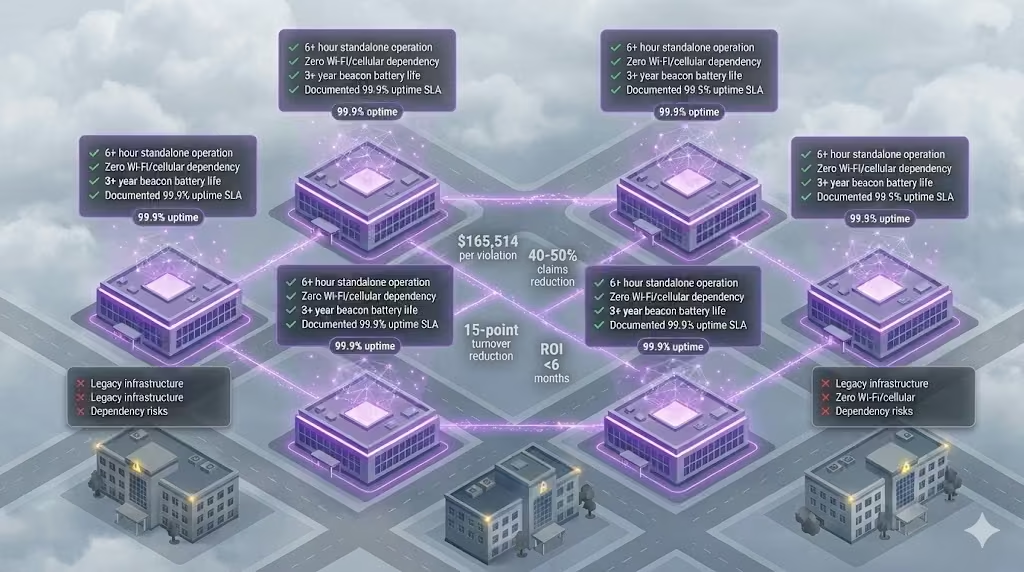
Four specifications now separate validated solutions from procurement risk: 6+ hour device operation, zero network dependency, 3-year beacon batteries, and documented outage performance with 99.9% uptime.
CTOs who require these standards position themselves as strategic enablers of operational resilience, defending their organizations against regulatory exposure and accreditation risks that follow system failures.
The Emerging Standard: What Peer Organizations Now Require
Enterprise health systems have begun requiring standalone power resilience as a procurement prerequisite—not a premium feature. In documented RFP cycles across behavioral health and integrated health systems, four specifications now appear as minimum requirements. Organizations still evaluating these capabilities as optional face a widening gap with peer institutions.
Healthcare workers face violence at five times the rate of other industries [1]. In behavioral health settings, 83% of nurses report experiencing violence in the preceding 12 months. Peer CTOs have recognized that the conditions generating incidents—storms, high-census events, infrastructure failures—are the same conditions that compromise Wi-Fi-dependent safety systems. This correlation has driven the shift toward standalone architecture requirements.
PEER STANDARDS
What are other CTOs requiring?
Four specifications now appear as minimum requirements in peer RFPs. See where you stand.
1. Device operation without building power: 6+ hours minimum. In one documented deployment at an integrated health system, a four-hour power outage produced zero coverage gaps because devices operated independently on battery. Fully charged devices demonstrated 6–8 hours of continuous operation.
3. Beacon battery life: 3+ years. Three-year batteries reduce total cost of ownership and eliminate rotating dead zones across multi-site deployments.
4. Documented outage performance: Real customer case studies. Validated solutions demonstrate 99.9% uptime verified by SLA, with 93% of incidents resolved in under two minutes. Customer retention rates of 99–99.5% on multi-year contracts signal sustained operational satisfaction.
The Gap: Where Most Organizations Fall Short
Organizations that have not updated procurement requirements face measurable exposure. The regulatory environment has shifted: $165,514 per willful OSHA violation [3], up to $75,000 per Joint Commission finding [4], and $2–5 million in annual funding at risk from accreditation loss.
The financial case peer organizations have used to close this gap centers on claims reduction data. Deployments demonstrate 40–50% reduction in workers’ compensation claims tied to violence and injury. At one behavioral health facility, claims decreased 24% in year one, contributing to a MOD score improvement of nearly 50%. A national behavioral health provider achieved 50% reduction in compensation claims within six months of deployment.
The turnover economics reinforce the business case. Each 1% reduction in RN turnover saves hospitals $263,000 annually in recruitment, training, and labor costs [5]. In one multi-site deployment, staff considering leaving due to safety concerns dropped from 22% to 7%—a 15 percentage point reduction in turnover intent. The cost to replace a single bedside RN reaches $61,110.
The capex efficiency supports straightforward approval. Documented deployments show $182 per staff member for complete solution implementation—a fraction of the $22,300 average cost per lost-time injury claim. Time to value under six months with 200% average first-year ROI provides board-defensible metrics.
Closing the Gap: How to Align with Peer Standards
When presenting to governance bodies, the peer-evidence approach proves effective. Leading health system technology leaders no longer evaluate power resilience as a premium feature—they require it as a procurement prerequisite, and their boards are approving the investment based on quantified returns.
Evidence from peer deployments warrants attention: standalone safety architecture operating during a documented four-hour facility outage with zero coverage gaps. Response times of 25–36 seconds for critical incidents. Customer retention of 99–99.5% across multi-year contracts.
A reasonable starting point: before the next contract renewal, validate current system behavior under simulated outage conditions. Disconnect facility power and Wi-Fi, then verify whether alerts still route to security. Document the results against the four specifications peer organizations now require.
WIDENING GAP
Peer CTOs already require this. Do you?
$165K per OSHA violation. $75K per Joint Commission finding. The standard has shifted.
The gap between organizations requiring these standards and those treating them as optional continues to widen. Peer CTOs who have adopted these requirements report stronger board support for safety infrastructure investments—the specifications provide objective criteria that shift the conversation from “should we invest more in safety?” to “does our current system meet the standard?”
Download the Power Resilience Benchmark Summary to share with your leadership team before your next vendor evaluation.
Most staff duress systems inherit the building’s power grid as a single point of failure, failing precisely when incidents spike during storms and infrastructure crises.
True resilience requires standalone architecture that operates for days without external power, not the hours most battery backup systems provide.
Four technical specifications separate systems that survive outages from systems that become liabilities during them.
During a 4-hour power outage at a Pennsylvania health system, the staff duress infrastructure continued operating without interruption. No coverage gaps. No manual workarounds. No scramble to protect staff in the dark.
That outcome was architectural, not accidental. And it exposes a vulnerability most CTOs have never evaluated in their current safety systems.
Staff rated the importance of rapid safety response at 4.75 out of 5 in pre-deployment surveys. Satisfaction with existing processes averaged only 3.55 (ROAR customer data). That gap exists because most safety infrastructure was designed for normal operations, not for the conditions when it matters most.
The Hidden Single Point of Failure You Haven’t Evaluated
Every technology system inherits dependencies. The question is whether those dependencies become single points of failure during crisis conditions.
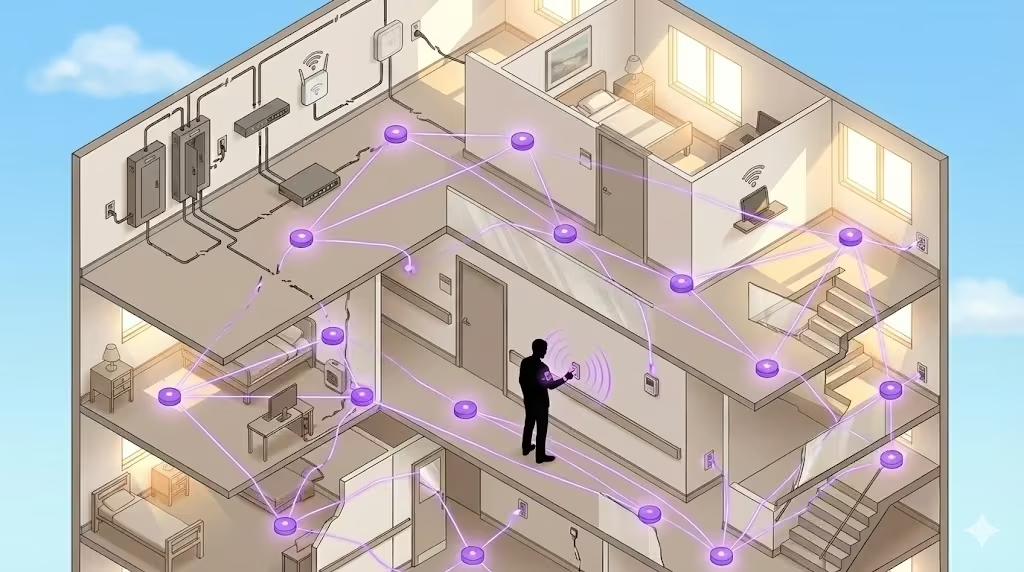
Most staff duress systems in behavioral health facilities share a common architecture: Wi-Fi or cellular connectivity routes alerts through the building’s IT infrastructure, which routes through the building’s power grid. When the grid fails, the entire chain fails. Fixed panic buttons mounted to walls require facility power. Wi-Fi dependent wearables require access points that require Power-over-Ethernet switches that require electricity. App-based solutions require charged phones and cellular signal.
This dependency chain creates a specific failure mode: the safety system fails at the moment when safety incidents are most likely to occur.
The architecture question CTOs rarely ask during RFP evaluation is this: what external dependencies does this system require to function? The answer for most legacy and first-generation wearable systems is facility power, network infrastructure, or both.
Consider the failure cascade during a typical outage. Power fails. UPS systems engage, providing minutes of bridge power. Generators activate. But the transition is not seamless for network-dependent systems. PoE switches reboot during the power transition. Wi-Fi access points cycle through startup sequences. Network authentication handshakes fail and retry. For a staff member facing an aggressive patient in a stairwell during this transition window, the duress button routes to nothing.
The infrastructure dependency is invisible during normal operations. Procurement teams evaluate systems during demonstrations on stable power. RFP responses describe battery backup as a feature without specifying whether backup addresses the actual failure mode. The gap between spec sheet claims and operational reality only becomes visible during the exact conditions when visibility matters least.
Healthcare workers face violence at rates five times higher than other industries [1]. Behavioral health settings concentrate that risk further: over 80% of behavioral health workers report being afraid a client would attack them, and more than one in four have called police or security for protection (ROAR industry data). The infrastructure protecting these workers should not share the same failure modes as the building’s HVAC system.
When Outages and Incidents Happen Together
Power outages and safety incidents are not independent variables. The conditions that cause one frequently cause the other.
Weather events create dual risk. Storms knock out power while simultaneously driving patient census spikes and stress-induced behavioral escalations. Grid instability creates facility anxiety while removing the safety infrastructure designed to manage that anxiety. Extended outages degrade environmental controls, increasing patient agitation in behavioral health settings where temperature regulation affects patient stability.
STANDALONE ARCHITECTURE
4-hour outage. Zero coverage gaps.
A Pennsylvania system kept staff protected through full power failure—no workarounds required.
The correlation extends beyond weather. Grid failures during peak demand periods often coincide with high-census conditions at facilities. Infrastructure stress events that trigger outages also trigger the staffing pressures and patient loads that elevate incident risk. The more severe the external crisis, the more likely both power failure and safety incidents become.
Emergency departments illustrate this convergence clearly. EDs are the most common site for active shooter incidents in hospitals, accounting for 30% of such events (ROAR industry data). They are also the areas most affected by census surges during community emergencies. The same events that overwhelm power infrastructure overwhelm emergency departments with trauma cases and behavioral escalations.
The correlation is structural. High-stress facility conditions that increase incident probability are often triggered by the same events that compromise power infrastructure. A safety system that fails during power loss is a safety system that fails during elevated risk periods.
Violence in healthcare is not evenly distributed across time. Incidents cluster around high-stress periods, shift changes, and environmental disruptions. The 81% of workplace violence incidents that go unreported (ROAR industry data) suggest that documented patterns understate the concentration of risk during crisis conditions. What gets reported represents the visible peak of a deeper pattern.
Healthcare violence costs U.S. hospitals $18.27 billion annually in turnover, liability, and treatment [2]. That cost concentrates in high-risk moments. A system that cannot operate during those moments provides coverage on a technicality, not protection in practice.
Why “Battery Backup” Isn’t Resilience
The phrase “battery backup” appears on most safety system spec sheets. It does not mean what most procurement teams assume it means.
Battery backup typically refers to UPS systems that maintain facility equipment during the transition to generator power. The window is measured in minutes, designed to bridge the gap until backup power activates. This is adequate for systems that can resume normal operation once generators come online.
Staff duress systems with Wi-Fi dependencies face a different problem. Generator power may restore the facility grid, but Wi-Fi access points often reboot during power transitions. Network switches reset. Signal propagation degrades during equipment restart cycles. The safety system may technically have power while functionally having no connectivity.
The terminology obscures the actual question. Battery backup describes a component. Standalone operation describes a capability. The component does not guarantee the capability.
Consider three failure scenarios that battery backup does not address. First, extended outages beyond UPS capacity: when generators fail or fuel runs out, systems dependent on facility power lose function regardless of backup specifications. Second, network equipment recovery time: even with continuous power, network-dependent systems require infrastructure restart before alert routing resumes. Third, partial facility failures: power may remain active in some building sections while failing in others, creating coverage gaps that facility-dependent systems cannot bridge.
The distinction matters for system specification. Battery backup sustains equipment through transitions. Standalone operation sustains functionality through extended outages without external dependencies.
The 4-hour outage at the Pennsylvania health system tested this distinction directly. The staff duress infrastructure operated continuously because it required no external power, no network connectivity, and no facility infrastructure to function. Wearable devices maintained 6-8 hours of battery life independent of any charging infrastructure. BLE mesh beacons operated on 3-year batteries, positioned throughout the facility without electrical connections. The mesh network routed alerts through neighboring beacons without Wi-Fi access points (ROAR customer data).
The self-healing mesh topology provided an additional layer of resilience. When one beacon loses function, signals route through neighboring beacons to reach the gateway. This eliminates single points of failure within the alert routing path itself, not just the power dependency.
That architectural choice, standalone operation versus infrastructure dependency, determined whether staff had protection during the outage or a compliance checkbox that offered no actual help.
The 4 Non-Negotiables for Standalone Safety Infrastructure
Your next staff duress system RFP needs four specifications. Without them, you are procuring liability, not protection.
1. Device operation without building power: 6 hours minimum.
Systems dependent on facility power fail during the exact conditions that trigger incidents. Storms, infrastructure failures, and high-census stress events increase both outage probability and incident probability simultaneously. In one documented deployment, a 4-hour outage produced zero coverage gaps because wearable devices operated on independent battery power with 6-8 hour capacity (ROAR customer data, UPHS).
The specification to require: wearable devices with 6+ hours of battery life that do not depend on facility power for operation.
2. Network independence: Zero Wi-Fi or cellular dependency.
If your staff duress system routes through IT infrastructure, your organization owns an outage risk that extends beyond power failures. Wi-Fi networks fail independently of power. Cellular signal varies by facility location. Router reboots during generator transitions create coverage gaps during the exact moments when staff need protection.
Short beacon battery life creates two operational problems. First, it creates maintenance burden on IT teams already stretched across competing priorities. Second, it creates rotating coverage gaps as beacons cycle through replacement schedules.
Three-year beacon batteries reduce total cost of ownership while eliminating the maintenance-driven coverage gaps that accumulate in systems requiring frequent battery replacement.
The specification to require: location beacons with 3+ year battery life and wire-free, peel-and-stick installation that does not require facility electrical connections.
4. Documented outage performance: Real customer case studies.
“Battery backup” is a spec sheet claim. Documented performance during actual outages is proof. The difference matters because real-world conditions expose failure modes that lab testing misses.
System uptime SLAs verified at 99.9% across deployments indicate operational reliability under normal conditions (ROAR metric). Documented outage case studies indicate reliability under abnormal conditions. Both matter for procurement evaluation.
The specification to require: customer reference calls that include discussion of system behavior during actual power outages, with specific documentation of duration and coverage continuity.
If your current system cannot meet all four specifications: You are one storm away from a coverage gap during a crisis. The gap between what staff need and what the system delivers becomes liability during the exact moments when protection matters most.
Start with a resilience assessment before your next renewal. Identify which dependencies your current system inherits and evaluate whether those dependencies create acceptable risk.
Testing Your System Before the Outage Tests You
Most facilities have never run a power outage drill on their staff duress infrastructure. The assumption is that battery backup and generator transition handle continuity. That assumption is testable.
A basic resilience test protocol for staff duress systems includes three scenarios that most IT teams can execute without vendor involvement.
First, test device function during facility power loss. Kill power to the area where staff duress infrastructure operates. Does the system continue to receive and route alerts? How long does coverage persist? Document the results against vendor specifications. This test reveals whether the system has true standalone capability or depends on facility infrastructure that the vendor describes as backup-protected.
Second, test network independence. Disable Wi-Fi access points in a test area while maintaining facility power. Does the staff duress system continue to function? If the system requires Wi-Fi connectivity, this test exposes dependency that power backup alone cannot address. Many systems marketed as having battery backup still route alerts through Wi-Fi, creating a dependency that survives power transitions but fails during network disruptions.
Third, test alert routing during transition. Simulate a generator transition by cycling power to network infrastructure. Document how long the safety system requires to restore full functionality after network equipment reboots. The gap between power restoration and alert routing capability represents unprotected time. In behavioral health settings where incident response targets sub-2-minute arrival, a 3-minute network recovery gap creates meaningful risk.
Beyond these basic tests, consider location accuracy verification during degraded conditions. Systems providing room-level location for responders may lose accuracy when beacons drop offline. Test whether partial beacon failure degrades location precision or creates blind spots in high-risk areas.
These tests expose operational reality versus spec sheet claims. The results inform procurement decisions for renewals and replacements. They also create documentation for compliance purposes, demonstrating due diligence in evaluating safety infrastructure resilience.
The testing protocol serves a secondary purpose: it forces vendors to clarify actual system behavior rather than describe aspirational specifications. A vendor confident in standalone architecture will welcome operational testing. Reluctance to support resilience testing suggests the system may not perform as claimed.
Staff safety rated at 4.75 out of 5 importance deserves infrastructure that performs at that priority level (ROAR customer data). Testing reveals whether current systems deliver on that priority or simply claim to.
What This Means for Procurement
The architectural question for staff duress systems is not whether the system has backup power. It is whether the system has standalone operation. The difference determines whether your organization has protection or paperwork during the moments when incidents are most likely.
Climate change is increasing the frequency of extreme weather events [3]. Grid instability is a structural trend, not an anomaly. Staff duress systems designed for infrastructure dependency inherit increasing risk as that dependency becomes more frequently tested.
The 4-hour outage case study demonstrates what standalone architecture looks like in practice: zero downtime, zero coverage gaps, zero manual workarounds. That outcome was not luck. It was the result of architectural choices made during system design.
Your next RFP should require those same architectural choices.
ONE STORM AWAY
Your next outage will expose the gap.
Battery backup ≠ standalone operation. Know the difference before renewal.
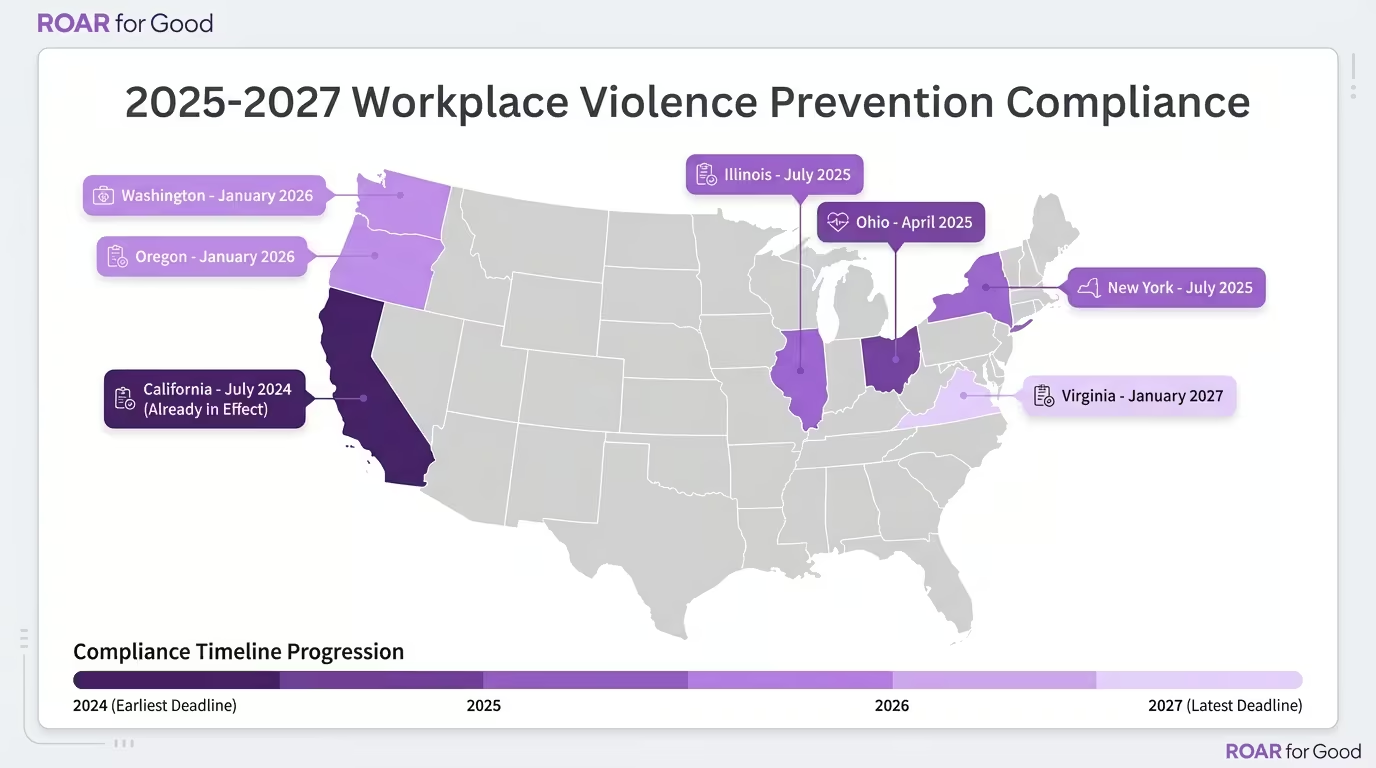
State workplace violence laws have shifted from advisory guidelines to enforceable mandates with real deadlines—Ohio’s requirements took effect April 2025, Illinois demands panic buttons by July, and nine more deadlines land before 2027.
Building infrastructure to meet the strictest standard (Illinois SB1435) automatically satisfies less prescriptive requirements in Ohio, California, Washington, and beyond—one investment covers the patchwork.
Getting ahead of the compliance wave protects your facilities from compounding penalties while positioning your system as a safety leader that attracts and retains staff.
The 2025 Enforcement Wave: What Changed
Until 2024, most state workplace violence laws were advisory or lacked enforcement teeth. That’s over.
Ohio became the first state to sign comprehensive hospital violence prevention into law on January 8, 2025, following a nurse’s death in Dayton [6]. Illinois followed with the nation’s first panic button mandate for hospital employees [2]. Washington enhanced its existing framework with annual plan reviews and detailed incident reporting [3].
The shift: requirements now come with deadlines, reporting obligations, and—in some cases—direct penalties for non-compliance.
2025-2027 Compliance Calendar
Deadline
State
Law
Key Requirements
April 9, 2025
Ohio
HB 452
Security plans, incident reporting, de-escalation training in ED/psych, employee input required [1]
July 1, 2025
Illinois
SB 1435
Panic buttons attached to staff ID cards for all hospital employees [2]
July 1, 2024
California
SB 553
WVPP for all employers, incident logs (5-year retention), annual training [7]
July 1, 2025
New York
A203
Violence prevention programs; security personnel in high-volume EDs [8]
January 1, 2026
Washington
HB 1162
Annual plan reviews, enhanced incident data reporting, safety committee oversight [3]
January 1, 2026
Oregon
HB 2552
Safety committees, incident data reporting to state, grant program for prevention [9]
January 1, 2027
Virginia
HB 1919
WVPP required for employers with 100+ employees [9]
TBD 2025-2026
Federal
OSHA Standard
Proposed rule for healthcare; comment period expected [10]
Pending
Federal
H.R.2531
Workplace Violence Prevention for Healthcare Workers Act—would mandate OSHA standard [5]
MULTI-STATE SYSTEMS
One investment. Every state covered.
OSHA fined a Florida healthcare company $100K+ in 2024—before any formal standard existed. Know where you stand.
OSHA fined a Florida healthcare company over $100,000 in May 2024 for violence prevention failures—using the General Duty Clause before any formal standard existed [10].
Illinois Sets the Standard: What Panic Button Mandates Mean
Illinois SB1435 is the first state law to explicitly require wearable panic buttons for hospital employees [2]. The bill amends both the University of Illinois Hospital Act and Hospital Licensing Act, requiring that all employees have a panic button attached to their staff identification card by July 1, 2025.
Why this matters for multi-state systems: Infrastructure deployed to meet Illinois requirements—wearable devices with location tracking and instant alerting—will satisfy the less prescriptive “prevention plan” requirements in Ohio, California, Washington, and other states. Building to the highest standard eliminates re-work as other states follow Illinois’s lead.
MULTI-STATE SYSTEMS
One investment. Every state covered.
OSHA fined a Florida healthcare company $100K+ in 2024—before any formal standard existed. Know where you stand.
The common thread across state requirements: rapid response, facility-wide coverage, and documented incident tracking.
Requirement Category
States Requiring
Infrastructure Solution
Written prevention plan
CA, OH, WA, TX, NY, VA
Plan development + technology documentation
Incident reporting/logs
CA, OH, WA, OR
Automated logging with 5-year retention
Employee training
All Tier 1 & 2 states
Integrated onboarding + annual refreshers
De-escalation personnel
OH (ED/psych), NY (high-volume ED)
Trained staff + alert routing to responders
Panic buttons/alert devices
IL (explicit mandate)
Wearable BLE devices with room-level accuracy
Safety committees with employee input
OH, WA, OR, PA (pending)
Committee reporting + analytics dashboards
Systems that deploy network-independent alert technology—operating without Wi-Fi or cellular dependency—satisfy the reliability requirements implied across all state frameworks while eliminating coverage gaps that create liability exposure.
Operating across multiple states? Contact us to map your compliance exposure and identify which requirements your current infrastructure already satisfies.
The behavioral health workforce shortage is a retention crisis disguised as a pipeline problem—19.2% of nurses leave after experiencing violence, and 60% have considered it.
One health system cut staff intent-to-leave from 22% to 7% not by recruiting harder, but by deploying safety infrastructure that delivers sub-2-minute response times.
Fixing safety fixes retention—and at $61,110 per lost nurse, the ROI on preventing exits dwarfs the cost of any recruiting campaign.
The workforce shortage conversation in behavioral health has been framed wrong for years. The dominant narrative centers on pipeline: not enough nursing school graduates, too few psychiatry residencies, aging demographics. All of these factors are real. None of them explain why you’re losing the nurses you already have.
The data tells a different story. According to the National Nurses United 2024 report, 19.2% of nurses have left their positions specifically after experiencing workplace violence [1]. That same study found 60% of nurses have changed jobs, left the profession, or considered leaving due to violence [1]. When nearly one in five departures trace directly to violence—and six in ten are considering the same exit—the math becomes inescapable. You cannot recruit your way out of a safety crisis.
The Violence-Turnover Math Most Workforce Strategies Ignore
Behavioral health facilities operate at the epicenter of healthcare violence. Industry data indicates 83% of mental health nurses experienced violence in the preceding 12 months. Over a career, between 24% and 80% of psychiatric nurses will be physically assaulted. Nurses in psychiatry face assault risk 20 times higher than their counterparts in public health units.
This violence does not stay on the unit. It follows staff into their decision to stay or leave. The 2025 NSI National Health Care Retention & RN Staffing Report places the average cost of replacing a single bedside registered nurse at $61,110 [2]. At that rate, every 1% reduction in RN turnover saves hospitals $289,000 annually in recruitment, training, and labor costs [2].
Consider what this means for a 100-nurse behavioral health unit. If 19.2% are leaving due to violence, you are hemorrhaging approximately $1.17 million annually in preventable turnover—before accounting for agency staffing premiums, overtime, reduced bed capacity, or the degradation of therapeutic continuity that comes with constant staff churn.
The recruitment machine cannot outpace this exit rate. As workforce analysts increasingly acknowledge, the traditional model is structurally broken. The supply pipeline cannot replace the experienced clinicians walking out the door.
The Intent-to-Leave Signal That Predicts Actual Turnover
Before nurses resign, they signal. Staff surveys consistently capture “intent to leave”—the percentage of employees actively considering departure. This metric is predictive. It is also actionable, which makes it far more valuable than tracking resignations after they occur.
In one multi-site health system deployment, a pilot study of wearable safety technology captured this leading indicator. Prior to the intervention, 22% of staff indicated they would consider leaving their positions due to safety concerns. This is not an abstract sentiment. These are employees actively weighing whether their physical safety justifies continued employment.
Four months later, that figure dropped to 7%. A 15-percentage-point reduction in retention risk—achieved not through wage increases or wellness programs, but through a single infrastructure decision: deploying a staff duress system that ensured help arrived in under two minutes.
The mechanism is straightforward. When staff feel unprotected, the psychological contract with their employer fractures. In documented customer environments, staff rated the importance of safety at 4.75 out of 5, but their satisfaction with existing safety processes averaged only 3.55 out of 5. That 1.2-point gap represents failed expectations. When organizations close that gap, retention follows.
Post-deployment, 76% of staff reported feeling “very prepared” to respond to an incident—up from 38% before implementation. Nearly 80% reported increased confidence in handling safety concerns.
What $61,110 Per Lost Nurse Actually Buys in Prevention
The comparison that reframes this conversation is not recruitment spend versus retention spend. It is the cost of inaction versus the cost of infrastructure.
Investment Comparison
Cost
Outcome
One RN departure
$61,110
Single replacement cycle (recruitment, hiring, orientation)
Staff duress system (per employee)
$182
Up to 38-point increase in safety sentiment; 15-point drop in intent to leave
These figures come from documented behavioral health deployments. The operating expenditure per staff member averaged $182. That investment delivered 200% average ROI in the first year across behavioral health facilities.
At one comprehensive behavioral health center, staff satisfaction rose from 57% to 73% within three months of deployment. The facility documented a 39% drop in violent incidents in the first quarter. Workers’ compensation claims declined 24%, driving their experience modification (MOD) score down nearly 50%—resulting in six-figure insurance savings.
The financial ROI compounds. Workers’ compensation claims for assault-related lost-time injuries average $58,000 per incident [3]. Documented customer facilities have achieved 40–50% reductions in claims post-deployment. The annual cost of workplace violence to U.S. hospitals reaches $18.27 billion—a figure that includes turnover, liability, and treatment [4].
The Regulatory Floor Is Rising
The business case for safety infrastructure now intersects with regulatory mandate. Illinois Senate Bill 1435, effective July 1, 2025, requires hospitals to ensure all employees have a panic button attached to their staff identification card [5]. This is not a recommendation—it is a licensing requirement.
The Joint Commission’s new workplace violence prevention requirements, also effective July 2025, mandate leadership oversight, reporting systems, and post-incident support across accredited facilities [6]. OSHA continues to enforce the General Duty Clause aggressively following violent incidents. Maximum penalties for willful violations now reach $165,514 per occurrence in 2025 [7].
Organizations that wait for a mandate or an incident to act face compounding risks: regulatory penalty, litigation exposure, and—most critically—continued workforce attrition during the delay. Joint Commission accreditation loss alone jeopardizes $2–5 million annually in Medicare and Medicaid funding for a typical hospital [6].
Retention Strategy Starts With the Staff You Already Have
The workforce shortage in behavioral health is real. The pipeline constraints are real. But the highest-leverage intervention available to CNOs and CHROs in 2025 is not a new recruitment campaign. It is preventing the 19.2% of departures that trace directly to violence.
The data from facilities that have made this investment is consistent:
Staff who feel protected stay. In one documented deployment, intent to leave dropped from 22% to 7%. At another behavioral health center, satisfaction rose 16 points in three months. Across multiple customer environments, staff safety sentiment has increased up to 38 points.
Response time determines outcomes. 93% of alerts across documented facilities result in help arriving in under two minutes. At one hospital, a response to an agitated patient occurred in 25 seconds, preventing escalation to a reportable assault.
Violence prevention pays for itself. The 200% first-year ROI documented across behavioral health deployments comes from a combination of reduced workers’ comp claims, lower insurance premiums, and avoided turnover costs—not from incremental efficiency gains.
The workforce strategy question for 2025 is not how to find more nurses. It is how to stop losing the ones you have. Violence is the preventable cause. Safety infrastructure is the available lever. The organizations that recognize this shift will stabilize their workforce. The organizations that continue to focus on recruitment alone will continue to watch experienced clinicians walk out the door—at $61,110 per departure.
Get Started
Ready to take the next step?
Schedule a personalized demo to see how our solution can help transform your business operations.
Behavioral health nurses face the highest violence exposure in healthcare, and when 22% of staff are considering leaving over safety concerns, the turnover math becomes catastrophic at $61,110 per RN departure.
Behavioral health organizations are shifting from individual training programs to infrastructure investments that cut violent incidents by 39% and slash intent-to-leave from 22% to 7% within months.
The result is a stabilized workforce, reduced workers’ comp claims by 40–50%, and a CFO-ready business case that reframes safety spending as retention strategy.
Your behavioral health nurses absorb more violence than almost any other role in healthcare. They’re also among your highest-turnover positions. These two facts are connected, and the connection is costing you far more than you’re tracking.
The average cost to replace a single bedside RN reached $61,110 in 2024, an 8.6% increase from the prior year [1]. In behavioral health settings, where violence rates dwarf general acute care, that number compounds rapidly. A 10-nurse departure over 12 months represents $611,100 in replacement, training, and productivity loss—before accounting for the institutional knowledge walking out the door.
The question CNOs and CHROs should be asking: how much of that turnover traces directly to safety?
The 22% Warning Sign
In behavioral health environments, staff don’t leave primarily for compensation or scheduling. They leave because they don’t feel protected.
Prior to deploying dedicated safety infrastructure, one behavioral health organization found that 22% of staff were actively considering leaving due to safety concerns [[2](ROAR Customer Outcomes)]. Not dissatisfaction with management. Not burnout from patient acuity. Safety—specifically, the perception that when something goes wrong, help won’t arrive fast enough.
That 22% figure aligns with national data. A 2024 survey from National Nurses United found that 19.2% of nurses had already changed or left their jobs due to workplace violence, with another 37.2% considering it [3]. In psychiatric and substance abuse settings, violence rates run more than 43 incidents per 10,000 full-time workers—among the highest of any healthcare environment [4].
When staff believe violence is inevitable and response is inadequate, intent-to-leave spikes. The downstream cost appears in your turnover reports six months later.
Why Individual Training Fails at Enterprise Scale
The standard response to nursing safety concerns is more de-escalation training. The logic seems sound: teach staff to manage volatile situations before they escalate.
The problem is that training addresses individual behavior, not system-level failures. When 81.6% of nurses report experiencing at least one form of workplace violence annually [3], and only 31.7% say their employer provides a clear way to report incidents [3], the gap isn’t skill—it’s infrastructure.
Consider what happens when a nurse faces an escalating patient in a stairwell at 2 AM:
De-escalation training provides verbal techniques
It does not summon a response team
It does not provide location tracking if the situation turns physical
It does not create a record for workers’ comp documentation
Training is a component of violence prevention. It is not a substitute for response infrastructure. Organizations that treat training as the primary intervention are solving for compliance, not outcomes.
What 39% Incident Reduction Looks Like Operationally
Behavioral health organizations that invest in dedicated duress systems—wearable panic buttons with real-time location tracking and guaranteed response times—see measurably different results.
One behavioral health provider documented a 39% reduction in violent incidents within the first three months of deployment [[5](ROAR Customer Outcomes)]. The mechanism isn’t complex: when staff can summon help with a single button press and responders know exactly where to go, situations de-escalate faster and incidents resolve before they become injuries.
The downstream effects compound:
Staff preparedness perception shifted from 38% feeling “very prepared” to handle safety incidents to 76% feeling prepared post-deployment [[6](ROAR Customer Outcomes)]—a 38-point swing that directly correlates with retention.
Intent-to-leave dropped from 22% to 7% [[2](ROAR Customer Outcomes)]. That 15-point reduction, applied to a 200-RN behavioral health workforce at the $61,110 per-departure benchmark, represents roughly $183,330 in avoided turnover costs annually.
Workers’ comp claims fell 40–50% in facilities with dedicated duress infrastructure [[7](ROAR Customer Outcomes)]. Given that the average medically consulted workplace injury costs $43,000 [8], the insurance savings alone often exceed the infrastructure investment within the first year.
Response times improved to under 2 minutes for 93% of alerts in ROAR deployments [[7](ROAR Customer Outcomes)]. Note: response times vary based on facility layout, staffing levels, and protocol design; some organizations see faster times while others may require additional optimization.
Building the Investment Case for Your CFO
The CFO conversation around staff safety typically stalls on ROI uncertainty. Safety investments get categorized as compliance costs rather than retention strategies, and budget allocation reflects that framing.
Reframe the ask. The relevant comparison isn’t “safety system cost vs. no cost”—it’s “safety system cost vs. turnover cost.”
Metric
Before Infrastructure
After Infrastructure
Financial Impact
Intent-to-leave (safety-related)
22%
7%
15-point reduction
Turnover cost per bedside RN
$61,110
$61,110
—
10-RN annual departure
$611,100
—
Avoided if retention improves
Workers’ comp claims
Baseline
40–50% reduction
~$43K per avoided claim
Incident response time
Variable
<2 minutes (93% of alerts)
Reduced severity, lower claim cost
The business case becomes straightforward: if your behavioral health network employs 200 RNs, and 22% are considering leaving due to safety concerns, you’re looking at potential turnover exposure of approximately $2.69 million annually (200 × 22% × $61,110 = $2,688,840). A 15-point reduction in intent-to-leave—demonstrated in actual deployments—changes the math entirely.
What CNOs Should Do Next
Calculate your current RN turnover rate and segment by exit interview reason. If safety concerns appear in more than 10% of departures, you have a retention problem masquerading as a safety problem.
Benchmark your response time data. If you can’t produce average incident response times by unit, you lack the infrastructure to demonstrate improvement—to staff, to the board, or to regulators.
Frame your next budget request around workforce stability, not security hardware. The CFO who won’t approve a “safety system” may approve a “retention investment” with documented ROI from peer organizations.
The $61,110 per-departure cost isn’t going down. The question is whether you address the safety perception driving turnover before or after your next budget cycle.
Get Started
Ready to take the next step?
Schedule a personalized demo to see how our solution can help transform your business operations.
Staff safety is no longer just a compliance box to check—it is now the single biggest factor in stopping nurses from walking out the door.
Leaders can finally bypass year-long IT delays by choosing wireless systems that protect staff instantly rather than waiting for complex installations.
This approach proves that protecting the budget and protecting your people are the same goal, securing finance approval without sacrificing care.
To the Enterprise CNO, the pressure is immense. You are tasked with leading staff, ensuring patient care, and managing budget, all while facing industry-high rates of violence across your network.
You know that violence damages morale, but the real cost isn’t emotional: it’s financial and existential.
The core problem is simple: Every safety failure pushes staff toward the exit, compounding your staffing shortage and increasing organizational risk.
Data confirms that 19.2% of nurses leave their positions specifically after experiencing workplace violence [2]. This leads directly to understaffing, which, in turn, creates a more volatile environment.
To break this loop, the CNO must treat safety as a strategic investment in retention, not just a cost.
Anchor Metric: The Cost of Inaction
The average cost of turnover for a single bedside RN is $61,110 [3]. For a multi-site network, a small safety-related turnover spike costs hundreds of thousands, quickly dwarfing the cost of intervention.
To win budget, the CNO needs a single solution that provides three strategic levers.
The Financial Lever: Stopping the Revenue Leak
When presenting to the CFO or Board, the CNO’s conversation must be about cost avoidance. You need solutions that directly mitigate liability and regulatory risk.
Ending the Claims Bleed
A passive response system allows incidents to escalate, leading to severe injuries and high-dollar claims (up to $58,000 per serious assault).
The Goal: Invest in systems that enable staff to intervene before violence occurs.
The Result: Behavioral health facilities have achieved a 40–50% reduction in workers’ compensation claims related to violence [8].
Securing Accreditation and Funding
Regulatory compliance is revenue protection. Non-compliance is expensive, threatening both fines and your ability to operate.
The Risk: Loss of accreditation status due to safety deficiencies can jeopardize $2–5 million annually per facility in Medicare/Medicaid funding [6].
The Standard: The CNO’s solution must provide auditable data to prove readiness for The Joint Commission and OSHA, reducing the risk of a willful violation fine of up to $165,514 [4].
The Operational Lever: Bypassing the IT Barrier
The CNO’s mandate is fast deployment, but IT integration creates the biggest project delay. Complex systems requiring cabling, server integration, and firewalls can stall critical safety projects for over a year.
The Strategic Pivot: Eliminate the integration barrier.
Focus on independent infrastructure that requires minimal IT support and avoids Wi-Fi dependency. Look for features that enable rapid deployment:
No Wiring: Battery-powered, “peel-and-stick” components (with anti-ligature safety devices for high-acuity environments).
Guaranteed Coverage: Patented mesh networks that ensure 100% coverage in stairwells and dead zones where facility Wi-Fi fails.
Time-to-Value: By bypassing infrastructure hurdles, systems can be deployed across multi-site enterprises in weeks, not months.
The Clinical Lever: Guaranteeing Confidence and De-escalation
At the point of care, safety equals speed. The goal is to move beyond passive alert systems (pagers, code phones, two-way radios) that lead to confusion and patient agitation.
Modern enterprise panic button systems must provide speed and reliability:
Fast reliability: Data shows that 93% of alerts receive a responder in under 2 minutes [7].
Silent De-escalation: Instant, discreet activation ensures help is on the way before an incident escalates further, empowering staff to safely de-escalate.
Reliability and speed directly contribute to staff morale, resulting in up to a 38-point increase in safety sentiment and dramatically improving nurse retention [7].
Conclusion: Leading with Enterprise Data
As CNO, you stand at the intersection of clinical quality and operational sustainability. You do not need to choose between protecting your budget and protecting your staff.
By framing workplace violence prevention through the lens retention ROI ($61k/nurse), regulatory assurance (100% audit pass), and claims reduction (20-50% drop), you build a business case that is bulletproof.
Safety is the foundation of care. It’s time to build it on a foundation of data.
Get Started
Ready to take the next step?
Schedule a personalized demo to see how our solution can help transform your business operations.
TLDR While federal guidelines like those from OSHA provide a foundation for WVP, a growing number of states — including California, New York, Illinois, Texas, Ohio, Oregon, and Washington — have enacted comprehensive laws requiring healthcare employers to implement violence prevention plans, conduct risk assessments, and train staff. Several more states advanced significant legislation in 2025, with new laws taking effect in 2026 and beyond. Healthcare employers must stay informed about state-specific regulations, develop tailored prevention strategies, and ensure that systems for reporting incidents are in place. By proactively addressing workplace violence and complying with state laws, healthcare organizations can protect workers and create safer environments.
“Violence in health care settings should never be accepted as “part of the job.”
States across the country are moving faster than ever to address workplace violence in healthcare settings. In the past two years alone, New York, Ohio, Oregon, Washington, Texas, and Virginia have all enacted new healthcare-specific workplace violence prevention laws — with comprehensive bills advancing in Massachusetts and Pennsylvania close behind.
The urgency is well-founded. Healthcare continues to top the list of industries where staff report intentional injury by others. The most recent federal benchmark — BLS’s 14.2 cases per 10,000 full-time workers in health care and social assistance — accounts for nearly 73% of all private-industry workplace violence cases, and available data suggests the rate has not meaningfully declined.
While federal agencies like OSHA, the CDC, and NIOSH provide overarching guidelines, it is state-level legislation that is driving the most concrete requirements and enforcement mechanisms. Here, I look to cover those states that are leading the way in improving protection for frontline healthcare workers with industry-specific laws and legislation. Read on to learn more.
While federal agencies like OSHA and the CDC provide essential guidelines for healthcare workplace safety, including the prevention of violence, it is the state-level laws that enforce and often expand upon these guidelines.
OSHA has been developing a healthcare-specific workplace violence standard (RIN 1218-AD08) for several years, with a Notice of Proposed Rulemaking initially targeted for June 2025. However, in late 2025, the agency moved this rulemaking to its “Long-Term Action” list, signaling that a binding federal standard is not expected in the near term. In the meantime, OSHA continues to enforce workplace safety in healthcare through the General Duty Clause and its 2015 voluntary guidelines.
At the state level, the picture is far more active. A growing number of states have enacted comprehensive workplace violence prevention laws tailored for healthcare settings, requiring hospitals and other healthcare institutions to develop written violence prevention plans, conduct hazard assessments, train staff, and establish policies for addressing incidents of violence. In 2025 alone, several states signed new healthcare WVP laws into effect, with more legislation advancing through committees.
State-Specific Workplace Violence Laws
With the rise of workplace violence now reaching untenable levels, I’m happy to see a number of states take the lead on improving working conditions. Below, I look at a variety of states and their specific approaches.
Alaska Senate Bill 49, prefiled in January 2025, would allow employers — including hospitals and healthcare organizations — to petition the court for a protective order on behalf of an employee who has experienced or been threatened with workplace violence. This law is intended to make it easier for healthcare institutions to proactively safeguard their workers from ongoing threats without requiring the individual staff member to file a petition themselves. As of April 2026, SB 49 remains pending in Senate Finance and has not been enacted.
California has one of the most comprehensive workplace violence prevention frameworks for healthcare settings in the country. The state’s healthcare-specific Cal/OSHA standard (Title 8, section 3342) requires employers to implement a workplace violence prevention plan that includes a risk assessment, hazard prevention methods, training programs, and a reporting system for incidents of violence.
In addition, Senate Bill 553 — in effect since July 1, 2024 — extends workplace violence prevention plan requirements to most California employers across all industries, including many healthcare employers beyond those already covered under section 3342. Cal/OSHA is currently developing a general-industry WVP regulation under SB 553’s mandate, with a final standard due by December 31, 2026, though as of early 2026, only drafts have been released.
Connecticut requires healthcare employers to annually prepare an assessment of factors that put employees at risk for workplace violence and develop and implement a workplace violence prevention and response plan in collaboration with the workplace. This core framework, established by Public Act 11-175 in 2011, remains in effect.
Connecticut has since expanded these protections significantly. Public Act 24-19 (2024) created detailed WVP requirements for home health care and home health aide agencies, including intake risk information, monthly safety assessments, staff training, and violence reporting. It also requires hospitals, behavioral health facilities, and other Medicaid-participating institutions to adopt workplace violence prevention standards aligned with Joint Commission or similar accrediting bodies. Public Act 25-168 (2025) extends these home health protections to hospice agencies, effective October 1, 2025.
Florida enacted House Bill 825 in 2023, signed by Governor DeSantis on May 24, 2023. Effective October 1, 2023, the law increases criminal penalties for assault or battery against hospital personnel statewide — not just in emergency departments. Under HB 825, assault against hospital workers is elevated to a first-degree misdemeanor, battery to a third-degree felony, and aggravated battery to a first-degree felony. No additional Florida healthcare-specific WVP prevention statutes (requiring plans, committees, or training) have been enacted as of April 2026.
Illinois has passed several state-level laws that require healthcare employers to implement workplace violence prevention programs, including risk assessments, employee training, and wearable staff panic buttons. The Healthcare Violence Prevention Act mandates that healthcare employers develop specific protocols for addressing violence and abuse within healthcare settings, including both physical and verbal assaults. This framework remains in full effect with no major amendments in 2025–2026.
Separately, SB 1435 would amend the University of Illinois Hospital Act and Hospital Licensing Act to require that hospitals provide all employees with a panic button attached to their staff identification card. While the bill specifies a July 1, 2025 effective date, SB 1435 was re-referred to the Senate Assignments Committee and has not advanced — the proposed effective date passed without action, and the bill remains pending as of April 2026.
Indiana Senate Bill 419, introduced in January 2025, sought to expand criminal penalties for battery against healthcare workers by making such offenses a Level 6 felony, with enhancements to Level 5 felony status when bodily injury or aggravating factors were involved. The bill passed the Indiana Senate in February 2025 but did not advance through the House Courts and Criminal Code Committee before adjournment. SB 419 is considered failed for the 2025 session.
Indiana does have a separate 2023 law (HEA 1021) that increased penalties for battery against emergency department staff, which remains in effect.
Massachusetts passed its foundational healthcare workplace violence prevention law in 2014, requiring healthcare facilities to develop violence prevention programs with staff training and security measures.
In 2025, the legislature advanced a significantly more comprehensive bill. Originally filed as H.2655, the legislation was redrafted as H.4767 and passed the Massachusetts House unanimously (158–0) on November 19, 2025. H.4767 would require healthcare employers to conduct annual facility-specific risk assessments, develop written WVP plans, provide training and post-incident support, report incidents annually to the Department of Public Health and district attorneys, and provide paid leave for workers seriously injured in workplace assaults. As of April 2026, H.4767 is pending in the Senate Committee on Ways and Means.
A separate proposal, H.2364, targets home healthcare settings, requiring employers to provide yearly safety training, communication devices, and the right to refuse unsafe assignments. H.2364 remains in committee with deadline extensions through June 2026.
Minnesota has specific workplace violence regulations for healthcare settings. Statute 144.566 requires hospitals to design and implement written preparedness and incident response action plans for violence against healthcare workers, with plans reviewed and updated at least annually.
The statute was strengthened in 2023 through SF 1384, which added a definition of “workplace violence hazards” and clarified requirements for employer review and staff involvement. Beginning January 1, 2025, hospitals must also submit their most recent action plan and annual review results to the Minnesota Department of Health, adding a state-level reporting element to the existing planning requirements.
New York signed Assembly Bill A203B (with Senate companion S5294B) into law on December 12, 2025 as Chapter 618 of 2025 — marking one of the most significant state-level healthcare WVP actions in recent years.
The new law requires general hospitals and nursing homes to establish workplace violence prevention programs consistent with CMS conditions of participation and accreditor standards. General hospitals must begin conducting annual safety and security assessments and developing security plans starting January 1, 2027. In jurisdictions with populations of one million or more, emergency departments must maintain at least one trained security guard or off-duty law enforcement officer on-site at all times. The law’s obligations phase in over the next two years, with full program implementation required within 12 months of the effective date (approximately September 2027).
New York also maintains enhanced criminal penalties for individuals convicted of assaulting healthcare workers, making it a felony offense in certain circumstances.
Ohio’s Healthcare Workplace Safety Act (House Bill 452) took effect on April 9, 2025, following Governor DeWine’s signature on January 8, 2025. The law was passed in the wake of a nurse’s tragic death in Dayton and requires hospital systems and stand-alone hospitals to establish formal security plans based on risk assessments, ensure at least one de-escalation-trained employee is present at all times in emergency and psychiatric departments, implement a workplace violence incident reporting system with anti-retaliation protections, and provide training for security personnel. Additionally, it mandates a survey of healthcare-related programs to assess current workplace violence training.
See how healthcare organizations are building compliance-ready safety infrastructure.
Oregon has strengthened its healthcare workplace violence prevention requirements through Senate Bill 537, signed by Governor Kotek on July 17, 2025 and effective January 1, 2026. SB 537 modernizes Oregon’s 2020 health care worker assault prevention law by requiring healthcare employers to develop comprehensive workplace violence prevention plans based on security assessments, maintain safety committees, conduct periodic assessments and annual training, and report workplace violence incidents to the Department of Consumer and Business Services. The law also expands the definition of covered workplace violence.
A companion House bill (HB 2552) covering similar ground did not advance and died in committee upon adjournment in June 2025.
Pennsylvania historically lacked a comprehensive healthcare-specific WVP statute, with hospitals relying on federal OSHA guidelines and internal policies. That is changing. House Bill 926, the Health Care Workplace Violence Prevention Act, passed the Pennsylvania House on May 6, 2025 (124–79) and was referred to the Senate Labor and Industry Committee, where it remains pending as of April 2026.
HB 926 would require hospitals, long-term care facilities, home health agencies, ambulatory surgical centers, birth centers, hospices, and psychiatric hospitals to establish violence prevention committees with substantial non-management representation, develop workplace violence prevention programs, implement reporting systems, and provide training and post-incident support.
Texas enacted Senate Bill 240 in 2023, creating one of the more detailed statewide healthcare WVP frameworks in the country. Effective September 1, 2023, with full compliance required by September 1, 2024, SB 240 requires a broad set of healthcare facilities — including hospitals, nursing facilities, home health agencies with at least two registered nurses, ambulatory surgical centers, freestanding emergency medical care facilities, and licensed mental hospitals — to adopt and implement written workplace violence prevention policies and plans. Facilities must also establish workplace violence prevention committees that include at least one RN, one physician providing direct care, and a security employee, and provide annual WVP training.
Virginia’s healthcare workplace violence legislative landscape shifted significantly in 2025. House Bill 1919, which would have required large employers to adopt workplace violence policies by January 2027, passed the General Assembly but was vetoed by Governor Youngkin on March 24, 2025. The House subsequently sustained the veto. A separate measure, House Bill 1620, which proposed forming a state work group to study workplace violence, was tabled in the House Rules Committee.
However, Virginia did enact new healthcare-specific protections through HB 2269/SB 1260, signed into law on March 24, 2025 and effective July 1, 2025. This law requires licensed hospitals to establish a workplace violence incident reporting system, document and analyze all reported incidents, provide at least quarterly reports to chief medical and nursing officers, and — beginning July 1, 2026 — submit annual data to the Virginia Department of Health. Hospitals must use this data to drive prevention improvements including de-escalation training, risk identification, and violence prevention planning.
Washington has enacted strengthened healthcare workplace violence prevention requirements through House Bill 1162, signed by the governor and effective January 1, 2026. Building on the state’s existing healthcare WVP statute (RCW 49.19), HB 1162 requires that workplace violence prevention plans be developed and overseen by safety committees with equal or greater employee representation, mandates annual reviews (previously every three years), and requires timely investigation of every workplace violence incident with findings reported to the relevant safety committee.
A Senate companion bill (SB 5162) was introduced but did not advance beyond committee referral; the enacted policy came through HB 1162.
Wyoming is considering House Bill 155, which would require every hospital, healthcare clinic, and long-term care facility receiving state funds to report workplace violence incidents against healthcare providers monthly to the Department of Workforce Services. The department would compile this data and report to the Joint Labor, Health, and Social Services Interim Committee. As of early 2026, the bill’s final enactment status has not been definitively confirmed.
How Healthcare Employers Can Ensure Compliance with State Laws
While legislation looks to catch up with rising levels of workplace violence, there’s plenty that healthcare employers can do to both address these issues and ensure they are on the right side of the law if legislation is passed.
Today, I think it’s crucial that employers take proactive healthcare policy initiatives to ensure compliance with state-specific workplace violence laws as well as reassess and improve on existing safety protocols. Start with the following and ensure that you regularly review your approach to WVP prevention.
Understand State Regulations — It is critical for healthcare employers to stay informed about the workplace violence prevention laws in the states where they operate. With new legislation taking effect in New York, Ohio, Oregon, Washington, and other states through 2026–2027, regularly reviewing local legislation ensures that organizations are aware of any changes that might affect their obligations.
Develop a Comprehensive Violence Prevention Plan — Healthcare employers should implement a workplace violence prevention plan tailored to their specific needs, incorporating risk assessments, safety protocols, and emergency response procedures. This plan should be regularly reviewed and updated to reflect new risks and changes in the legal landscape. States like California, Ohio, Oregon, and Texas now mandate annual plan reviews.
Employee Involvement — Including healthcare workers in the development and execution of the violence prevention plan ensures that the strategies are effective and address real-world concerns. Staff should be trained regularly on de-escalation techniques, emergency response procedures, and how to report incidents of violence. Multiple new state laws — including Pennsylvania’s pending HB 926 and Ohio’s HB 452 — specifically require non-management representation on WVP committees.
Create a Safe Reporting System — Establishing a confidential and accessible reporting system for employees is essential in addressing workplace violence. Healthcare workers should feel empowered to report incidents without fear of retaliation. Virginia’s new HB 2269 specifically mandates that hospitals track, analyze, and report workplace violence data at both the institutional and state levels.
Monitor and Evaluate the Plan — Healthcare employers should regularly monitor the effectiveness of their violence prevention programs. This includes tracking incidents, assessing the success of preventative measures, and making adjustments as necessary.
“Workplace violence is going unreported because people feel that there is no effective system in place to make the effort of reporting it worthwhile,” Dr. Lebares said. “People don’t expect anything to be done about it.”
Healthcare-specific violence prevention strategies are crucial for addressing the unique risks faced by healthcare workers. These strategies focus on identifying potential hazards, providing the necessary training, and ensuring that healthcare facilities are equipped with the appropriate safety measures to prevent and respond to violent incidents effectively. By tailoring approaches to the healthcare environment, these strategies help create safer workspaces for both staff and patients.
Hazard Evaluation — Identify risk factors like patient behavior, staffing levels, and facility layout. Multiple state laws now require annual facility-specific risk assessments as a baseline compliance step.
Staff Training — Provide training on de-escalation techniques and recognizing warning signs of violence. I also recommend building a robust and supportive safety culture in any healthcare facility.
Security Assessments — Regularly assess facility security to ensure adequate safety measures. Ohio’s HB 452 requires at least one de-escalation-trained employee present at all times in emergency and psychiatric departments.
Safety Measures — Ensure the installation of staff duress systems, alarms, surveillance cameras, and proper security personnel. New York’s new law mandates trained security presence in high-volume emergency departments.
Emergency Preparedness — Train staff on procedures for responding to violent incidents and emergencies.
Conclusion
State-specific healthcare workplace violence prevention laws are essential to improving the safety and security of healthcare workers. With major new laws enacted in New York, Ohio, Oregon, Washington, Texas, and Virginia — and comprehensive bills advancing in Massachusetts and Pennsylvania — the regulatory landscape is shifting rapidly. Healthcare employers must stay informed about the legal landscape, ensure compliance, and adopt tailored violence prevention strategies. By doing so, they can create a safer work environment, reduce incidents of violence, and improve the overall quality of care.
COMPLIANCE
Build a Safer, Compliant Workplace
ROAR's staff duress system is already helping healthcare organizations across the country meet evolving state mandates and protect their frontline workers. A short conversation can show you what that looks like for your facility.
In February 2021, landmark legislation was introduced to the Senate directing the Secretary of Labor to issue occupational safety and health standards across the healthcare and social service industries. Its purpose: to address the shocking levels of violent and antisocial behaviors that leave healthcare workers five times more likely to be injured than workers in any other industry, and to ensure that comprehensive workplace violence prevention plans are standardized across healthcare and social services.
While data suggests that up to 38% of healthcare workers suffer physical violence at some point in their careers, a recent study published by the The Joint Commission Journal on Quality and Patient Safety highlights how proxy measures used to represent workplace violence (WPV) lead to underestimation and underreporting. Put simply, post-event restraint, incident, and injury reports fail to accurately record the true number of violent, aggressive, and antisocial incidents within the industry, and by shifting reporting to event counters, staff in the study were exposed to 1.17 events per 40 hours worked.
As a company deeply committed to improving the lives of workers most at risk, we have long recognized the need for more and better data that represent the true levels of WPV within the healthcare industry. We believe no one should be afraid while trying to earn a living, and understanding the broader picture of WPV while ensuring that proper incident reporting systems are in place are crucial to create safer workplaces for all stakeholders.
With these thoughts in mind, this article aims to gather some of the existing data from a variety of sources to paint a comprehensive view of WPV within healthcare settings. Read on to learn more and explore our suggestions on how to develop strategies designed to reduce incidents.
1. Overview of Aggressive Incidents
There is little argument that violent and aggressive incidents have risen significantly since the COVID-19 pandemic; however, WPV was undoubtedly an issue before, and data is taken from as far back as 2011. Here are some of the most striking stats that help build an overview of the true levels of aggressive incidents within the healthcare industry.
An NNU survey reported that 26.3% workplace violence had increased in the past year (2022-2023) and 81.6 percent have experienced at least one type of workplace violence,
2. Quantifying Aggression: A Statistical Overview
Violent, aggressive and antisocial workplace incident statistics must also quantify the types of aggressions and to whom they were directed. These data highlight how verbal aggressions underpin all types of WPV, and how they can escalate into more serious incidents.
6 in 10 RNs report having changed, left, or considered leaving their position due to workplace violence with, 19.2% specifically citing “changed or left job” on Table 5 of this NNU survey on page 15.
3. Understanding the Triggers of Aggression
Understanding the factors that trigger aggressive behaviors in patients is key to identifying when, where, and how WPV incidents play out. These data aim to shine a light on some of those triggers.
By some estimates, 75% of healthcare workers do not feel safe at work, and healthcare facilities stand to lose an average of $37,000 to $58,400 per staff turnover. Combined, these statistics suggest that all stakeholders within healthcare facilities stand to benefit from safer workplaces—the staff subject to WPV, the facility’s ROI, and the patients that stand to lose better levels of care when staff are intimidated or threatened.
One such facility that stands at the forefront of innovation in the provision of treatment services for individuals with substance use and mental health challenges, is The Behavioral Wellness Center at Girard in Philadelphia. ROAR was privileged to introduce a 3-month pilot at the facility that aimed to improve incident response and de-escalate incidents through the use of wireless panic buttons in tandem with existing CCTV and other WPV solutions.
During the pilot, these statistics were noted:
A 39% reduction in incidents between patients and staff and a significant upswing in staff peace of mind.
Worker compensation claims decreased by 24% when compared to the facility’s historic claims rate.
A 50% reduction in the overall MOD score.
Staff satisfaction increased from 57% to 73% once rollout was complete.
5. Management Strategies in Response to Aggression
Verbal De-escalation Techniques — 75.2% of events within the Joint Commission’s report were de-escalated using verbal techniques, and it remains one of the most powerful tools within healthcare professionals’ arsenal. Active listening, empathy, and the use of non-confrontational language are key, as well as clear, calm, and reassuring communication. The Crisis Prevention Institute has excellent resources on these topics.
Physical Environment Modifications — The environment in which healthcare professionals work and patients receive care can have notable effects on behaviors, with overcrowded areas a particular flashpoint. This means that the physical environment should be designed with clear sightlines and unobstructed pathways, as well as including safe areas for staff retreat during emergencies. Additionally, access controls, security cameras and panic button systems can all help improve existing environments that may not have these options.
Staff Training and Education — Ensuring staff are well educated on how to recognize warning signs of escalating aggression is key to addressing WPV and ensuring incidents are dealt with in the least damaging ways possible. Education on verbal intervention and conflict resolution are critically important, as well as simulation exercises to practice responding to violent incidents, and cross-training staff from different departments to support each other during emergencies.
Documentation and Reporting — As part of a WPV prevention plan, and by harnessing all available data documenting incidents that includes near-misses and close calls, reporting incidents correctly and in a timely fashion is another important management strategy. Data analysis should aim to identify trends and patterns for targeted interventions, such as during medication administration or when patients are waiting for care. Additionally, qualitative reporting on the nature of incidents can allow organizations to provide better aftercare and support for employees subject to WPV.
Policy Development and Enforcement — Establishing clear policies and procedures for managing aggression and regularly reviewing and updating policies in response to changing circumstances are both core elements of a comprehensive WPV plan. Additionally, it is important to enforce consequences for violations of workplace violence policies.
Technological Solutions — Panic buttons for summoning immediate assistance are increasingly becoming required by law for lone and vulnerable workers across the US. In addition, they can help provide quantitative and qualitative data on WPV, sometimes in tandem with video surveillance systems for monitoring and deterring violence, access control systems to restrict entry to high-risk areas, and integrated communication systems for coordinated responses.
6. Legal Considerations and Implications
Today, the Occupational Safety and Health Act of 1970 remains the core piece of legislation in the fight against workplace violence, and its approach to WPV is insufficient and out-dated. However, efforts are underway to bring in federal legislation designed to tackle workplace violence specifically within healthcare and social services, providing a much needed refresh on strategies to address WPV head-on.
Both the SAVE Act (Safety from Violence for Healthcare Employees), and the Workplace Violence Prevention for Health Care and Social Service Workers Act are currently being considered within the Senate. Additionally, OSHA provides comprehensive information on workplace violence within healthcare settings, encouraging the development of solid workplace violence prevention programs.
At the state level, California has introduced the broad-reaching Workplace Violence Prevention Act that stretches across all industries and sectors. This will come into force on July 1st 2024, and requires all employers to establish, implement, and maintain an effective written Workplace Violence Prevention Plan. Additionally, various state laws have been enacted within the hotel and hospitality industry that require establishments to introduce panic button systems or personal safety devices, alongside other WPV measures intended to address rising levels of aggression.
Data on the prevalence and impact of WPV in the post-pandemic world continues to grow, with this latest study revealing higher levels of incidents than previously accounted for, with event-counter reporting providing a new perspective on violent and aggressive incidents. For now, the healthcare industry waits on legislation designed to tackle these issues, meaning that non-comprehensive measures and inconsistent WPV plans will remain a significant hurdle to improving safety. Ultimately, legislation must standardize the approach to tackling WPV issues and ensure that healthcare facilities are doing all they can to reduce, minimize, and control all violent and aggressive behaviors for the sake of all stakeholders.
For more information on how ROAR’s staff duress solutions can help your facility protect their staff, contact us today or request a demo.
Connecting Life-Saving Data to 911 with a Push of a Button
Over the past several years workplace violence incidents have increased at an alarming rate. In a wide-ranging study conducted by the Bureau of Justice Statistics (BJS), the Bureau of Labor Statistics (BLS), and the National Institute for Occupational Safety and Health (NIOSH) between 1992 and 2019, there was a staggering 25% increase in nonfatal incidents of workplace violence, accounting for 9.2 violent crimes per 1000 workers.
With the increase in these daily threats to workers comes the need for safety solutions to protect employees, ones that call for help quickly, accurately and provide people with access to life-saving help. Since 2013 ROAR has been providing these life-saving solutions to people across a variety of industries including healthcare and hospitality with a dual-patented panic button technology that creates a field of safety in and around facilities, ensuring help is called exactly when and where it is needed. Continuously innovating to address the rising threat to employees, ROAR looked to RapidSOS, a world-class 911 intelligent safety platform for further enhancement functionality to the ROAR panic button solution.
Every day, RapidSOS connects life-saving data from 540+ million devices across industries to over 1 million first responders. RapidSOS software is used by 99% of 911 centers across the country supporting over 171M emergencies in 2023. Built alongside public safety, RapidSOS has over 500 years of combined public safety experience. Given this best-in-class solution, RapidSOS was the ideal partner to collaborate with in development of the ROAR 911 panic button solution.
“We implemented 911 functionality based on feedback from our customers who wanted to ensure their workers were able to receive emergency response help. The ROAR panic button provides workers with the ability to call 911 quickly, efficiently and with 100% reliability. Whether it’s for a medical emergency, a workplace violence incident, or a robbery, the ROAR 911 panic button provides a lifeline for staff adding a layer of security to your facility,” said ROAR co-founder and CEO Yasmine Mustafa. “Our mission is to empower people through technology to create safer organizations, and this new launch enables us to do just that, quickly and easily.”
According to RapidSOS Chief Revenue Officer, Indranil Chatterjee, “RapidSOS and ROAR are united in our commitment to empowering safer, stronger communities with intelligent, data-driven emergency response worldwide. Together with our RapidSOS Ready Emergency Community, we’re providing people with an added layer of safety and security, and we’re supporting our heroic first responders across 171 million emergencies annually.”
How it Works
ROAR’s 911 Panic Buttons call for help with a simple press and hold the button, providing the employee’s exact location, site phone number and entry instructions to RapidSOS’s call center. Beyond location information, RapidSOS also supports sharing emergency intelligence data to increase the amount of data first responders can obtain during a call. This empowers faster and more effective emergency responses and provides first responders with the critical information they need to protect lives.
Providing an added layer of protection for at-risk workers across a variety of industries including healthcare and hospitality, ROAR + RapidSOS give employees peace of mind knowing that their calls for help are escalated to emergency services quickly without reaching for a phone.
Healthcare—Healthcare providers can utilize ROAR’s panic buttons in a variety of locations as they provide care to their patients. They can be invaluable for doctors’ offices, labs, rehabilitation centers, women’s reproductive clinics, health centers providing gender affirming care, and numerous other settings.
Behavioral health—Therapists, counselors, and psychologists often find themselves in one-on-one working environments with their patients. It is estimated 1 in 4 mental health workers have called the police for protection from a client. Additionally, psychiatric wards, mental health facilities, and addiction treatment centers can benefit to protect front line workers who may be at risk of dangerous outbursts or physical attacks.
Hotels— This can apply to front-desk staff, room attendants, housekeepers, maintenance personnel, and valets who are often alone or isolated.
A wide variety of workplaces now benefit from ROAR’s 911 panic button solution, including a retail chain in New York City with a large volume of foot traffic, multiple hotels serving Anaheim, CA’s biggest tourist attractions like Disneyland and the Convention Center as well as recovery centers, mental health providers, and medical facilities throughout the U.S.
ROAR Panic Button Solutions offer unwavering protection for employees, guests, and visitors. Your safety is our mission. To learn more: [Get a Demo]
Professionals in the healthcare industry suffer a disproportionately high number of violent events and physical injuries in the workplace. According to the Occupational Safety and Health Administration (OSHA), 2016 saw U.S hospitals record 228,200 work-related injuries and illnesses, a rate of 5.9 work-related injuries and illnesses for every 100 full-time employees. That’s around twice the rate of private industry as a whole. The Covid-19 pandemic seems to have made the situation worse, with some parts of the country seeing violence against health workers increase by a shocking 300%.
In order to prevent violence and improve workplace safety, employers and managers need to take concrete steps to keep their doctors, nurses, and healthcare workers safe. While violent incidents are unlikely to disappear overnight, creating a more secure work environment will help professionals to feel safer and enable them to care for patients to the best of their abilities.
Workplace Violence in Healthcare
Violence in the workplace has long been a problem in healthcare facilities across the country. In fact, in many areas, the issue is so bad it’s now become viewed simply as “part of the job”.
According to a recent study, 70–74% of workplace assaults in the USA occur in healthcare settings. Among staff in nursing homes and residential care facilities, the rate of violent incidents is around 10 times the national average. While those working in psychiatric and substance abuse hospitals experience violence at roughly 60 times the rate of the average US workplace.
Types of Workplace Violence in Healthcare
According to the CDC, there are four main types of workplace violence in healthcare. These are criminal intent, client-on-worker violence, worker-on-worker violence, and violence from personal relationships.
Criminal intent
Criminal intent refers to violence that’s committed by someone with no known links to, or relationship with, the healthcare setting or its employees. It could include a nurse being attacked in the parking lot on her way home or a doctor being mugged when conducting a home visit. In general, this type of violence is fairly rare.
Client-on-worker
This is the most common type of violence experienced by healthcare workers. The client in this context includes the patient, their family members, and their friends. Those most likely to experience this type of violence are emergency department workers and those working in mental health facilities, waiting rooms, and geriatric care.
Worker-on-worker
Violence between co-workers is also known as lateral or horizontal violence. It can include everything from bullying and intimidation to emotional abuse and homicide.
Personal relationship
The violence that comes about as a result of personal relationships can happen in all healthcare settings. An example of this type of violence would be a husband following his nurse wife to work and attacking her on the hospital premises.
Causes of Workplace Violence in Healthcare
The causes of workplace violence in healthcare vary from place to place and incident to incident. As we’ve seen, violent events can fall into four broad categories, with each presenting its own risk factors and triggers.
However, while the exact causes of violence can’t always be identified, policies and programs that target violent behavior can be effective in addressing workplace incidents of violence. For example, the integration of rapid response programs and technologies has the potential to reduce the severity of incidents as they happen, while de-escalation training can be incredibly useful in defusing situations that may arise once a qualified member of staff has arrived.
Lack of Reporting
While the causes of workplace violence in healthcare settings are nebulous and often facility specific, a lack of reporting compounds the problem—regardless of the challenges faced by individual facilities. Put simply, when violence against healthcare workers goes unreported, the ability to address and prevent future incidents effectively is negatively affected. Under reporting or neglecting to report incidents in a timely manner may have the following consequences:
Inadequate Data
Lack of reporting leads to incomplete or inaccurate data regarding workplace violence incidents in healthcare facilities. This makes it difficult for organizations to fully understand the scope and severity of the problem, affecting the ability to allocate resources and implement appropriate preventive measures.
Underestimation of the Issue
When incidents of workplace violence are not reported, there is a risk of underestimating the magnitude of the problem. Without a clear understanding of the frequency and severity of violent incidents, organizations may fail to prioritize and allocate sufficient resources for workplace violence prevention initiatives.
Missed Opportunities for Intervention
Reporting incidents of workplace violence is crucial for prompt intervention, enabling organizations to identify patterns, assess risk factors, and implement preventive measures to address the root causes. Without proper reporting, opportunities to intervene and prevent future incidents may be missed.
Prolonged Exposure to Risk
Failure to report workplace violence incidents prolongs the exposure of healthcare workers to potentially dangerous situations and individuals. This increases the risk of further violence, placing employees at continued risk and potentially compromising their safety and well-being.
Impacted Workplace Culture
Lack of reporting can contribute to a culture of silence and acceptance of violence in the workplace. Employees may feel discouraged or fearful of reporting incidents due to concerns about retaliation or a perception that their concerns will not be taken seriously. This negatively impacts the overall workplace culture and hinders efforts to create a safe and respectful environment.
Various Risk Factors of Workplace Violence in Healthcare
These risk factors primarily relate to client-on-worker violence, the most common type of violence experienced by those working in healthcare organizations, and it is crucial to identify, educate, and monitor these risk factors to increase safety within the healthcare industry. This can be achieved by implementing the following:
Workplace Analysis and Hazard Identification
Conducting a thorough analysis of the healthcare facility’s work environment is crucial in identifying potential hazards and risks that could lead to incidents. This analysis involves evaluating the physical layout of the facility, identifying high-risk areas, assessing staffing levels, and considering factors such as access control, lighting, and visibility.
Safety and Health Training
Providing comprehensive training programs for all employees is vital to promote a safe work environment and prevent workplace violence. Training should cover topics such as recognizing warning signs, effective communication and de-escalation techniques, personal safety strategies, and protocols for reporting incidents. Ongoing workplace violence prevention programs and refresher courses should be conducted to ensure that employees are well-prepared to handle challenging situations.
Record Keeping and Program Evaluation
Keeping detailed records of incidents, near misses, and employee reports is essential for tracking patterns and trends related to workplace violence. This data can be used to evaluate the effectiveness of prevention measures and identify areas that require improvement. Regular program evaluations should be conducted to assess the overall effectiveness of workplace violence prevention strategies and make necessary adjustments to enhance the safety of the healthcare environment.
Tips and Strategies for Preventing Workplace Violence in Healthcare
These simple measures can have a big impact on the level of violence experienced by staff members. Implementing an emergency communication system, and ensuring healthcare professionals undergo relevant training programs, can also have an instant and significant impact on physical assaults and threatening behavior. In addition, these strategies can help prevent and mitigate workplace violence in healthcare settings.
Participate in Your Facility
Take an active role in workplace safety by participating in safety committees, attending training sessions, and providing input on policies and procedures. Collaborate with colleagues and management to develop and implement violence prevention programs.
Dress for Safety
Wear appropriate attire that allows for ease of movement and quick identification as a healthcare professional. Avoid clothing or accessories that may provoke or escalate aggressive behavior.
Be Aware of Your Work Environment
Stay alert and be aware of your surroundings at all times, familiarize yourself with escape routes, emergency exits, and panic buttons, and report any safety hazards or concerns promptly to management.
Be Aware of Patient Behaviors
Pay attention to changes in individual behaviors and be mindful of warning signs that may indicate escalating aggression or potential violence. This can include verbal threats, physical aggression, agitation, or signs of substance abuse or withdrawal.
Use Violence Risk Assessment Tools
Implement violence risk assessment tools or checklists to identify individuals who may be at a higher risk of displaying violent behavior. These tools can help healthcare professionals evaluate the likelihood of violence and develop appropriate preventive measures.
Check Your Socio-Cultural Biases
Be mindful of your own biases and stereotypes that may influence your perception or response to certain individuals or situations. Treat individuals with respect and fairness, regardless of their background or personal characteristics.
Further resources on workplace violence prevention can be found on The Joint Commission website and in the OSHA guidelines, as well as by following this NIOSH link from the CDC.
Do you Need a Workplace Violence Program?
Violence against healthcare workers is always completely unacceptable. Implementing workplace violence prevention programs can help to reduce violence in a number of ways. Programs can provide essential training for healthcare workers and can be used to inform employees and employers about the steps they can take to reduce assaults and minimize risk.
Whether or not your healthcare facility has experienced violence, investing in a program is an important way of boosting security. It also demonstrates to employees that their safety is a top priority, something that can further help to improve the working environment.
Behavioral health is a serious issue across the U.S. According to a 2021 study, an incredible one in five Americans lives with a mental illness, while one in ten experiences a drug use disorder at some point. In the last few years, the Covid-19 pandemic and opioid health crisis worsened the situation. The World Health Organization (WHO) estimates that the pandemic alone triggered a 25% increase in the prevalence of anxiety and depression worldwide.
However, despite the profound need for mental and behavioral health services, there’s a chronic shortage in the behavioral health workforce. According to recent figures, nearly half of the U.S. population – 47% or 158 million people – live in a mental health workforce shortage area. This means that almost one in two Americans aren’t getting the care and support they need to get their lives back on track.
Why Is There a Shortage in the Behavioral Health Workforce?
Mental illness and substance use disorders are key factors in disability, mortality, and healthcare costs. So, it’s essential that Americans have good access to behavioral and mental health professionals. At the moment, however, things only appear to be getting worse. According to current projections, by 2030, there will be a 20% decrease in the supply of adult psychiatrists and a 3% increase in demand for their services. This makes psychiatry one of the leading mental health professional shortage areas.
There are several reasons behind the current behavioral health workforce shortage. One of the most important revolves around Medicaid. Figures show that demand for mental health services is highest among Medicaid enrollees. Around 39% of people on Medicaid suffer from behavioral or mental health issues.
However, only 36% of psychiatrists accept new Medicaid patients (compared to 71% of physicians). Moreover, even those who accept new Medicaid patients often take just a few, leaving millions without access to mental and behavioral health practitioners.
Many people are also put off from entering the profession because of poor security and high workplace violence rates. Up to 80% of mental health nurses and more than 40% of other mental health care clinicians experience violence at some point in their careers.
How Workplace Safety Is Contributing to the Shortage
High levels of violence in the mental health care sector directly contribute to the behavioral health workforce shortage. Not only does workplace violence put people off from entering the profession, but it can also negatively impact staff retention rates, further reducing the number of behavioral health providers available.
Repeated studies have shown that exposure to workplace violence is associated with poor mental health outcomes and unfavorable physical and emotional performance. Long-term exposure to workplace violence has been shown to lead to higher levels of PTSD, burnout, anxiety, depression, and insomnia in the mental health workforce.
Examples of Concerns Unique to the Behavioral Health Field
Many of the concerns held by behavioral health workers aren’t unique to the sector. However, they are amplified by regular exposure to patients with serious mental illness and substance abuse disorders. For example, many – even those outside the health system – are concerned about violence in the workplace. Many are also worried about a lack of funding and lack of provision.
However, these concerns are brought to the fore in the behavioral health field because mental health care professionals, especially those on the frontline, are far more likely to experience violence than other workers. In addition, people suffering from severe, acute mental illness and substance abuse issues are more prone to erratic behavior. This can lead to violent and aggressive outbursts.
Impact of Safety on Recruitment and Retention Efforts
If social workers, family therapists, and other mental health providers don’t feel safe in the workplace, they’re less likely to stay in the profession for an extended period. Studies have shown that exposure to workplace violence directly leads to poor mental health and high burnout, stress, and anxiety levels. These, in turn, result in high staff turnover.
As well as retention rates, safety concerns can make it difficult for healthcare providers to recruit staff in the first place. This can lead to fewer professionals joining the healthcare workforce.
Possible Solutions to the Workforce Shortage
There are several complex reasons behind the workforce shortage in the behavioral health sector. However, some solutions can help to address some of the most common issues impacting behavioral health workers.
Examples of Technological Solutions, Such as Wearable Devices and Alarm Systems
Technological solutions can help reduce workplace violence and make mental health professionals and primary care providers feel safer when treating their patients. For example, electronic entry systems can be used to control who enters and exits a building, and CCTV can be put in place to help security personnel better monitor the premises.
Duress systems are another good option for mental health treatment centers. These systems can be installed in patient rooms and communal areas, or mental health workers can be issued with wearable devices (also known as panic buttons). One of the benefits of wearable devices is that they’re always on hand when workers need them. So if a clinician feels that their safety is at risk, they can trigger the wearable device and get help as quickly as possible.
Discussion of Best Practices for Implementing Safety Technology in the Workplace
Because all psychiatry and primary care settings are different, there’s no ‘one size fits all’ solution regarding safety technology in the workplace. Talking to staff about their concerns, and analyzing any prior incidence of workplace violence, is the best way to find the most effective solution.
Improved safety in the workplace benefits everyone, so it’s important to ensure all employees are involved in the implementation process. Instead, a collaborative approach will ensure all workers are comfortable with the safety solutions and that everyone is aware of the measures taken.
Advocate for Policy Change
Advocating for policy change is one of the most effective ways of improving the situation long term. For example, if the Department of Health, public health bodies, and policymakers legislate for better funding, prompt Medicare payments, higher reimbursement rates, and investment in safety technology, the real, permanent change could be achieved across the sector.
Retaining current behavioral health professionals is a big piece of the puzzle when tackling the workforce shortage. Human services departments, government agencies, and state legislatures can employ many methods for improving retention rates in the behavioral health sector.
Better Compensation and Benefits
Increasing compensation and benefits for psychiatrists, mental health workers, and clinical social workers can help to stop professionals from leaving the sector. Studies have shown that raising pay helps to improve satisfaction levels and increase staff retention.
Professional development
Offering professional development opportunities can also help to improve levels of staff satisfaction. For example, internships, placements, specialist courses, and initiatives incentivize existing team members and help overall workforce development.
The Substance Abuse and Mental Health Services Administration (SAMHSA) lists a number of professional development opportunities. In addition, the Health Resources and Services Administration (HRSA) also offers information on development programs. These are focused on high-need communities, such as pregnant people, children, low-income households and communities in rural areas.
Improve Working Conditions
Improving working conditions is key to boosting retention rates. Offering peer support, professional support specialists, and a safer workplace can help workers to feel happier and more appreciated.
More flexible working can also help to improve behavioral health conditions for workers. For example, giving professionals the chance to provide telehealth services instead of face-to-face consultations, can make it easier for people to work from home and achieve a better work-life balance.
Want to discover how our wearable, affordable, silent panic button solution will help you lower workers’ comp claims and boost profitability while keeping your people safe? Request a Demo.