Your quality committee tables safety technology when peer outcomes arrive as clinical data rather than the oversight metrics they already track and act on
Peer psychiatric facilities document assault reductions, faster response times, and workforce stability gains that map directly to quality indicator categories your committee reviews
A bounded pilot on one high-risk unit gives your committee a measurable decision point, reducing organizational risk while building the evidence base internally
Your clinical safety brief keeps stalling. You brought peer outcome data to the quality committee twice. Both times, the committee acknowledged the evidence, asked clarifying questions, and moved the item to next quarter’s agenda. The data was solid. The framing missed. Governance audiences table clinical evidence when it arrives in a language they can’t act on.
Why Clinical Conviction Stalls Internally
Psychiatric and substance abuse hospitals face the highest workplace violence rate in healthcare: 110.4 incidents per 10,000 workers [1]. Your quality committee likely knows this. The number describes a clinical problem, and committees approve governance actions. That gap is where your brief dies.
Boards tracking performance through focused quality dashboards with governance-aligned metrics produce better outcomes than those reviewing broad clinical data [2]. The pattern holds for quality committees. When safety evidence arrives as a clinical concern, it competes with dozens of other agenda items. When it arrives as a governance metric tied to accreditation, workforce stability, or regulatory compliance, it gets a different hearing.
No one should face violence while trying to help others heal. The shift you need is a different frame around the evidence you already have.
Framing Peer Outcomes for Governance Audiences
Three translation moves convert your peer clinical data into language committees act on:
Clinical outcome → quality oversight metric. A 40% assault reduction is a clinical outcome. Reframe it: “Comparable psychiatric facilities documented a 40% reduction in assault frequency, tracked as a process quality indicator alongside response time and reporting infrastructure.” Now it fits the quality dashboard.
Safety improvement → regulatory compliance lever. Joint Commission accreditation loss risks suspension of Medicare and Medicaid funding worth millions annually for typical hospitals [3]. Connect peer safety outcomes to Joint Commission’s 2022 workplace violence prevention standards, and the committee hears compliance risk reduction. For additional peer evaluation framing, the CMO Peer Evaluation Guide maps these connections in detail.
Staff safety → workforce stability. At one ROAR deployment, staff who said they’d consider leaving due to safety concerns dropped from 22% to 7% [4]. That single metric is simultaneously a safety outcome for you, a retention number for your CEO, and a financial data point for your CFO. Lead with whichever version matches your audience.
Peer Data Your Quality Committee Needs
Quality committees evaluate three indicator types: structural, process, and outcome. Your clinical safety brief should map peer data to all three.
Indicator Type
What It Measures
Documented Peer Outcome
Process
Incident response speed
93% of incidents resolved in under 2 minutes
Outcome
Assault frequency change
40% reduction within six months at a comparable psychiatric facility
Structural
Reporting infrastructure
Most nurses lack a clear, reliable way to report incidents
Peer outcomes sourced from ROAR deployment data [4].
Present these as trending categories. Your committee reviews dozens of items per meeting. A brief that maps to their existing indicator framework gets read. A brief that requires them to build a new mental model gets tabled.
Your physicians will push back. Prepare documented responses:
“This will disrupt the therapeutic milieu (the treatment environment).” Safety is foundational to all other treatment: no intervention works when safety is compromised [5]. One peer medical director reported zero disruption to patient care or additional workload during deployment [4].
“We already have de-escalation training.” De-escalation training reduces aggression. Technology covers what happens after prevention: the response gap training leaves open.
“This will add workflow burden.” Workflow burden ranks below funding and privacy concerns as an adoption barrier in behavioral health [6]. Your CNO can confirm that staff satisfaction at peer facilities improved after deployment.
A behavioral health safety specialist can help you map peer outcomes to your committee's indicator framework.
Ask for a bounded measurement period rather than system-wide commitment.
Define the pilot in terms your committee already approves: one high-risk unit, defined duration, three success criteria the committee selects in advance. Decision-makers approve bounded commitments with clear governance checkpoints far more readily than open-ended investments [7]. Staff preparedness at one pilot site doubled, jumping from 38% to 76% within the evaluation period [4].
This pilot structure works best when the quality committee defines success criteria before deployment begins. Committees that define criteria after seeing results introduce selection bias into the governance review.
At the end of the measurement period, the committee reviews the data and decides on expansion. They approve a familiar governance action.
Safety should be a promise, not just a priority. You now have a clinical safety brief built for the audiences that approve investments. The peer data categories, the reframing techniques, the objection responses, and the bounded pilot ask are ready for your next quality committee meeting. The translation, the part that stalled your committee, is handled. You have the brief, the reframes, and the ask.
PEER EVIDENCE
Ready to Present Your Clinical Safety Brief?
See the documented outcomes from psychiatric facilities comparable to yours, framed for governance review.
Jiang HJ, Lockee C, Bass K, Fraser I. Board oversight of quality: any differences in process of care and mortality? Journal of Healthcare Management, 2009. https://pmc.ncbi.nlm.nih.gov/articles/PMC3876189/
Your quality committee needs peer clinical safety outcomes filtered through evidence criteria, with limitations documented, before they can act on any safety initiative recommendation
The evidence filtering step belongs to you personally as CMO because grading methodology, identifying bias, and assigning confidence levels requires clinical judgment that can’t be handed off
A completed peer outcome summary serves every future quality committee meeting, medical staff discussion, and survey preparation cycle when you update it quarterly
Your quality committee needs a peer clinical safety outcomes summary they can evaluate with the same rigor they apply to any clinical intervention. Here’s why that’s urgent: behavioral health facilities face 110.4 violent incidents per 10,000 workers, the highest rate in healthcare [1]. That rate is exactly why quality committees demand structured evidence rather than undocumented peer impressions.
This guide walks you through producing that deliverable: peer facilities matched to your clinical profile, outcomes filtered through evidence criteria, and limitations documented alongside every result.
What Clinical Outcome Collection Accomplishes
This process produces one deliverable: a reusable summary your quality committee can review with the same rigor they apply to any clinical intervention.
Quality committees expect evidence across three categories. The NIH framework defines them as [2]:
Quality committees require specificity across all three categories that only documented peer data can provide.
What does structured peer data look like in practice? Facilities with documented safety technology report 93% of incidents resolved in under two minutes [3]. That’s a process metric with a defined measurement method (system-generated alert logs) and a clear threshold. Your quality committee can evaluate it. An informal peer report about “faster response times” lacks the measurement method and threshold your quality committee needs to evaluate it.
Think of it like the difference between a lab result and a hallway opinion. One has a methodology your committee can assess. The other doesn’t.
Verification question: Can you name the three evidence categories your quality committee reviews when evaluating a new intervention?
Prerequisites for Credible Peer Evaluation
Before collecting a single peer outcome, confirm three things are in place.
1. Your own baseline metrics. You need your facility’s current numbers for restraint rates, staff injury rates, incident frequency, and staff safety sentiment scores. Without these, peer outcomes have no comparison point. Staff retention concerns related to safety are widespread across behavioral health. If you haven’t measured sentiment at your own facility, you can’t evaluate whether a peer’s improvement is meaningful for your environment.
2. Facility matching criteria. Match peers on at least three of these five variables:
Matching Variable
Why It Matters
Acuity level
Higher-acuity facilities have fundamentally different incident profiles
Bed count
Scale affects staffing ratios and response logistics
Patient population
Forensic, adolescent, and adult units produce different baselines
Clinical staffing model
Nurse-to-patient ratios shape both incident rates and reporting rates
Reporting systems
Facilities with clear reporting systems capture more incidents, inflating baseline numbers
3. Evidence standards you’ll apply. Decide before you start: What methodology qualifies? What timeframe is credible? How will you grade confidence? Having these criteria defined prevents the committee from questioning your standards after the fact.
Verification question: Can you state your facility’s current restraint rate and staff injury rate for the past 12 months?
For multi-site systems: a 200-bed acute psychiatric hospital and a 40-bed residential treatment center need different peer comparisons. Build a facility-level matching table showing which peers correspond to which internal sites.
Four Steps to Evaluate Peer Clinical Safety Outcomes
Step 1: Identify matched peers
Use your three-to-five matching criteria to select two to four peer facilities. ROAR’s network provides a documented peer outcome set across 350+ behavioral health facilities [3]. Your CNO and CSO may already have peer contacts. Coordinate to avoid duplicating outreach.
Step 2: Collect specific metrics
For each peer, gather:
Incident reduction rate with timeframe
Response time data with measurement method
Staff safety sentiment with survey methodology
Workers’ comp trends with comparison period
Step 3: Apply evidence filters
This step requires clinical judgment that belongs to you personally.
Walk through each peer outcome and ask: What was the measurement methodology? What was the timeframe? What’s the sample context?
Here’s how that works. One national behavioral health provider documented a 40% reduction in staff assaults within six months [3]. That’s a pre/post comparison with a defined window. Grade it as customer-reported pre/post data, credible as a reference point, pending independent verification. A second facility reported 39% reduction in three months. Two facilities showing similar magnitude across different timeframes strengthens confidence, but both carry the same limitation: vendor-reported customer outcomes.
Verification question: For each peer outcome in your summary, can you identify the measurement methodology, timeframe, and confidence grade?
When Peer Data Falls Short
Three limitations show up in nearly every peer outcome summary. Document each one alongside your results. Transparency strengthens the summary. Omitting caveats undermines it.
Underreporting bias. Roughly 81% of workplace violence incidents go unreported [4]. Every peer outcome you evaluate sits on incomplete data. Note this: “Peer outcomes reflect reported incidents only. Actual incident volumes may be higher at both peer and comparison facilities.”
Reporting systems variation. Only 31.7% of nurses say their employer provides a clear way to report incidents [5].
Facilities with better reporting systems capture more incidents, which can make their baseline numbers look worse. When one facility reports a 50% workers’ comp reduction and another reports 24% [3], the gap may reflect timeline, facility size, or baseline severity rather than intervention quality.
Missing outcome data. The vast majority of behavioral health outcomes carry high risk of bias from missing data [6]. Missing outcome data is a documented challenge across behavioral health research, peer-reported and published alike. Name it so the committee sees you’ve accounted for it.
Verification question: Have you noted underreporting risk and reporting systems variation alongside every peer outcome?
A behavioral health safety specialist can help you identify matched peer facilities for your evidence collection.
Cross-check against your own data. Does the summary include your facility’s baseline metrics alongside peer outcomes? The quality committee needs to see the comparison alongside the peer numbers.
Verify regulatory alignment. Joint Commission standards require organizations to define and collect data on performance measures relevant to patient safety [7]. Accreditation loss risks suspension of Medicare and Medicaid funding [7]. Your summary must meet this documentation floor. Work with your compliance team to confirm it does.
Confirm evidence thresholds. Every peer outcome should have a methodology note, timeframe, confidence grade, and documented limitations.
Task
Who Owns It
Compile baseline metrics
Delegate to Quality Officer and site medical directors
Identify peer facilities
You approve matching criteria; delegate outreach
Apply evidence filters
You personally. This requires your clinical judgment.
Draft limitation notes
Delegate drafting to Quality Officer; you review for clinical accuracy
Verify regulatory alignment
Delegate to Corporate Compliance; you sign off
Compressed timeline: If your quality committee meets in under two weeks, match two peers on acuity and bed count only. Use published deployment data (40% assault reduction at six months, 39% at three months) as reference points. Flag clearly: “Preliminary summary. Full five-criteria matching to follow in Q[next]. Vendor-reported outcomes included pending independent verification.” Deliverable in five to seven business days.
Your summary is ready. It meets the same evidence standards you apply to any clinical intervention. You don’t need to perfect it before presenting. Start with what you have, then update quarterly as new peer data becomes available.
The process is yours to repeat for every clinical safety outcomes discussion ahead. One summary at a time.
PEER EVIDENCE
Ready to Build Your Peer Evidence Summary?
See the documented clinical outcomes from behavioral health organizations comparable to yours.
Healthcare accreditation surveys test whether your violence prevention program works — not just whether it exists on paper. These FAQs cover what Joint Commission surveyors evaluate, where facilities get cited, how different leaders prepare, and why staff duress deployment changes the evidence equation during accreditation visits.
What do Joint Commission surveyors actually evaluate in a violence prevention program?
Surveyors assess four evidence categories: staff awareness, response capability, incident tracking, and leadership accountability. They walk units, interview frontline staff, and pull random incident records to trace follow-through — they do not sit in a conference room reviewing policy binders. The gap between having a program and proving it works on demand is where most citations start. Surveyors can tell within minutes whether your evidence reflects active operations or last-minute compilation.
Why do strong violence prevention programs still fail accreditation surveys?
Programs fail surveys because of documentation gaps, not missing protocols. A facility can have excellent de-escalation training and fast response times, but if those outcomes are not captured in retrievable records, surveyors treat them as unverified claims. More than 80% of workplace violence incidents go unreported, which means incident logs often understate what actually happens on units. Surveyors compare staff interview answers against documented records, and inconsistencies trigger deeper scrutiny.
What are the most common citation risks during behavioral health surveys?
The two dominant citation categories are inadequate training records and leadership oversight failures — each flagged in more than half of behavioral health surveys with violence prevention findings. Other common risks include investigation trails that stop at the initial report, multi-site inconsistency in protocol execution, and underreporting that makes incident logs look artificially low. Night-shift and weekend staff who cannot articulate protocols are a frequent surveyor exploit point.
How quickly do surveyors expect facilities to produce evidence?
Surveyors expect response time data, system reliability records, and coverage verification within 30 minutes of a request. Investigation records and training documentation typically fall within a 24-hour window. Facilities with automated systems pull dashboards in seconds, while manual programs often spend hours compiling spreadsheets and hoping the gaps are not obvious. That speed difference shapes the entire tone of the survey conversation.
What specific questions do surveyors ask frontline staff?
Surveyors ask staff to describe what they would do during a violent incident, how they would call for help, what happened after the last incident they witnessed, and whether they feel the organization responds to reports. These questions test whether protocols live in daily practice or only in training binders. A charge nurse on night shift gets the same questions as a day-shift manager, and a locum who started last week gets the same questions as a ten-year veteran. Staff answers must be consistent across roles, shifts, and sites.
Who owns what during accreditation survey preparation?
The CEO owns delegation and governance proof, not protocol details. The CMO coordinates across clinical leadership to verify physician and staff competency documentation. The CNO ensures unit-level evidence is producible across all shifts, and the CSO owns response capability and system reliability records. Survey readiness breaks down when everyone assumes someone else owns a deliverable. A named delegation table with specific owners, deliverables, and timelines prevents that failure.
How does staff duress deployment technology change survey outcomes?
Automated systems generate timestamped response data, continuous monitoring proof, and coverage verification as a byproduct of daily operations. Facilities with documented safety technology show 93% of incidents resolved in under two minutes — a number that ends surveyor follow-up questions immediately. These facilities produce evidence that already exists rather than compiling it under pressure. The result is that survey readiness becomes continuous instead of episodic.
How should leaders handle the anxiety of an upcoming survey?
Survey anxiety usually comes from knowing your program works but not being sure your records can prove it. That gap between operational confidence and documentation confidence is real, and it affects CNOs, CSOs, and CEOs differently. The fix is building systems where evidence generates automatically through daily use so preparation sprints become unnecessary. When any record is producible in under 30 minutes, the survey window stops feeling like a threat.
What financial consequences follow accreditation loss?
Accreditation loss can suspend Medicare and Medicaid billing immediately, putting millions in annual revenue at risk for behavioral health systems. OSHA penalties for willful workplace violence violations now exceed $165,000 per violation. Beyond direct financial exposure, boards need to see accreditation protection framed as risk mitigation alongside program effectiveness and workforce stability data.
How do peer-leading organizations prepare differently for surveys?
Peer-leading programs generate evidence continuously rather than compiling it before a survey window opens. Their security directors open dashboards instead of flipping through binders. Their CNOs can pull five random incidents and show complete investigation trails on demand. The clearest benchmark is evidence speed — how long it takes to produce incident trending data when a surveyor asks. Organizations that pass surveys with confidence are not better at preparing; they are better at making preparation unnecessary.
What is the single best test to check survey readiness right now?
Pull your incident trending data for the past 90 days. If that takes more than 30 minutes, your evidence infrastructure has a gap surveyors will find. Then ask a night-shift charge nurse to walk through your violence response protocol without checking any reference materials. Those two tests — evidence speed and staff demonstration capability — reveal more about your readiness than any policy review.
Does higher incident reporting hurt or help during a survey?
Higher documented incident counts actually strengthen your position with surveyors. Facilities that report more incidents demonstrate an active reporting culture, which surveyors value far more than artificially low numbers. When 81% of incidents go unreported industry-wide, low counts signal underreporting rather than safety. Surveyors look for trending data that reflects actual acuity levels paired with complete investigation follow-through on every reported event.
How should multi-site systems handle consistency across facilities?
Multi-site inconsistency is one of the most common citation risks in behavioral health surveys. Surveyors expect the same protocols, documentation standards, and staff competency levels at every location. Corporate offices typically own policy standards, but each facility must demonstrate local execution with its own evidence. Automated systems help because they enforce the same data capture process everywhere, eliminating site-by-site variation in how records are generated.
What should a CEO present to the board about survey readiness?
Present documented outcomes across three lenses: risk mitigation, program effectiveness, and workforce stability. Show response time data, incident trending over six months, staff confidence metrics, and investigation completion rates — not policy summaries. Each data point should connect to a financial consequence the board already tracks, like OSHA penalty exposure or RN turnover costs. If you cannot pull any of those numbers today, that gap is what needs to be fixed before the next board meeting.
How far in advance should survey preparation start?
Survey preparation should not start at all — it should already be happening. The most effective programs treat evidence generation as a daily operational function, not a pre-survey sprint. For organizations closing gaps, a 90-day action sequence covers the highest-priority items: export testing, investigation trail audits, night-shift readiness checks, and governance reporting verification. Mock surveys conducted during that window can reduce official findings by 20–30%.
More than half of behavioral health surveys with violence prevention findings cite training gaps, and over half cite leadership oversight failures, making these the two highest-risk areas for accreditation.
Documented outcome data from facilities with safety technology shows measurable response times, incident reduction, and pass rates that satisfy what surveyors evaluate.
A CMO evidence portfolio covering response capability, incident trending, training competency, and governance reporting provides the survey-ready documentation that policy binders alone can’t deliver.
About 56% of behavioral health surveys with violence prevention findings cite inadequate training records. Another 55% cite leadership oversight gaps [1]. These aren’t edge cases. They’re the two most common reasons behavioral health facilities run into trouble during accreditation visits. This staff duress deployment data brief compiles the outcome evidence that demonstrates program effectiveness when surveyors come looking for proof.
The Citation Pattern
The data tells a consistent story. The most common citation category involves training records that prove attendance but not competency [1]. Sign-in sheets show who was in the room. Surveyors want evidence that staff retained what they learned and can demonstrate it on the spot.
Leadership oversight gaps follow close behind. Surveyors look for board reporting, leadership rounding observations, and executive participation in program development [1]. When those records are missing or inconsistent, the citation targets leadership accountability rather than frontline performance.
Underneath both patterns sits an underreporting problem that makes the numbers worse. 81% of workplace violence incidents go unreported by healthcare workers who experienced them [2]. Only about a third of nurses say their employer gives them a clear way to report [3]. Behavioral health settings face the highest violence rates in healthcare, with psychiatric facilities seeing roughly 11 times the incident rate of the general workforce [4]. When surveyors interview staff who’ve experienced violence but see no corresponding records, the gap reflects directly on program credibility.
Facilities with documented safety technology produce measurable outcomes that map directly to what surveyors evaluate. The data shows consistent patterns across tracked deployments:
Evidence Category
Documented Outcome
Why It Matters
Inspection results
100% Joint Commission and OSHA pass rate [5]
Direct accreditation evidence from facilities with systematic tracking
Response capability
93% of incidents resolved in under 2 minutes [5]
Quantified response data replaces anecdotal estimates
Incident reduction
39% reduction in patient-staff incidents within 3 months [5]
Measurable program effectiveness over time
Staff preparedness
Staff feeling “very prepared” increased from 38% to 76% after deployment [5]
Training effectiveness with before-and-after data
The practical difference matters. When a surveyor asks how quickly help arrives, pulling a report showing documented response times with historical trending ends the conversation. An estimate invites follow-up questions that get harder with each one.
Behavioral health facilities show 40% reduction in assaults against staff within six months of deployment [5]. That trajectory matters for CMOs building internal business cases: the same data that satisfies surveyors demonstrates ROI to the board.
The Financial Stakes
Accreditation loss can suspend Medicare and Medicaid billing, putting millions in annual revenue at risk for behavioral health systems [6]. OSHA penalties for willful workplace violence violations exceed $165,000 per violation [7]. Beyond penalties, the regulatory exposure includes CMS reviewing compliance with its own standards when Joint Commission accreditation lapses [8].
But the financial case extends past risk avoidance. Each percentage point change in RN turnover costs roughly $289,000 annually [9]. Facilities with documented safety systems report measurable improvement in staff feeling safe at work [5], and that connection between documented safety and retention is the number that resonates with CFOs and boards.
Want to see what documented outcome evidence looks like for your facilities?
Training competency: pre-training and post-training assessment scores for all staff, including travelers and agency nurses. Attendance records without competency proof are the single most cited gap [1].
Investigation follow-through: complete trails from incident report through root cause analysis, corrective action, and resolution for every documented event. Surveyors pull 5-10 random incidents and review each trail [10].
Governance reporting: quarterly safety data presented to leadership with evidence of discussion and follow-up action.
Behind the 81% underreporting rate are staff who’ve experienced violence and concluded that documenting it changes nothing. Systematic documentation changes that calculation by making every incident visible and every response measurable. For CMOs, the staff duress deployment data compiled here provides the evidence that surveyors evaluate and that policy binders alone can’t deliver.
SURVEY EVIDENCE
Build Your Evidence Portfolio Before Surveyors Arrive
Facilities with documented safety systems produce the outcome evidence surveyors evaluate. See what that looks like for your organization.
Documentation-only approaches have structural limitations that create gaps surveyors are trained to identify, regardless of how thorough the policies are.
Technology-generated evidence addresses those gaps by producing timestamped, continuous records that match what surveyors specifically request.
A comparison matrix mapping documentation vs. technology evidence across six surveyor criteria helps CMOs assess where their current approach falls short.
Every behavioral health CMO faces the same question before an accreditation visit: does your evidence show that your violence prevention program works, or does it show that the program exists? The distinction matters because surveyors evaluate implementation through documented outcomes, not policy binders. This staff duress deployment comparison examines what each evidence type actually provides and where the gaps live.
Documentation Evidence: What It Shows and Where It Falls Short
Documentation-based approaches establish that a program exists. Policies are written, training is scheduled, incident forms are available. For surveyors, that’s the starting point, not the finish line.
The core limitation is structural: manual records depend on staff to document incidents during or after crisis moments. 81% of workplace violence incidents go unreported by healthcare workers who experienced them [1]. Only about a third of nurses say their employer gives them a clear way to report [2]. When staff focused on de-escalation don’t stop to log timestamps, records capture what people remember afterward, not what actually happened.
That gap compounds across every evidence area surveyors assess:
Evidence Area
What Documentation Provides
Where It Falls Short
Response capability
Anecdotal estimates reconstructed after incidents
No timestamped data showing how fast help actually arrived
Incident tracking
Reports filed by staff who chose to document
Misses the majority of incidents that go unreported
Staff readiness
Sign-in sheets proving training attendance
No evidence that staff retained or can demonstrate what they learned
No proof the system was operational between checks
The limitations aren’t about effort. Security directors and CNOs working with manual systems aren’t doing it wrong. The system itself can’t capture what it depends on humans to record during the moments they’re least able to do so.
Technology Evidence: What Automated Systems Produce
Technology-generated evidence addresses the structural gap by capturing data as incidents happen rather than relying on post-incident documentation. The practical difference shows up in three areas surveyors specifically evaluate:
Timestamped response data. When a surveyor asks how quickly help arrives, facilities with automated systems pull documented response times with historical trending. Facilities with documented safety systems show 93% of incidents resolved in under 2 minutes [3]. That’s a different conversation than “we respond quickly.”
Continuous monitoring proof. Surveyors request 90-day trending data as a minimum for analysis [4]. Automated systems generate this continuously, analyzed by unit and shift. Manual compilation of the same data after a survey is announced creates gaps in detail and consistency that surveyors notice.
Coverage verification. Surveyors walk facilities including stairwells, parking structures, and utility areas [4]. They check whether staff can summon help from every location. Automated systems document coverage across the full facility including outdoor areas. Manual approaches rely on assumed coverage that hasn’t been verified since the last walkthrough.
Facilities with documented safety technology have passed every Joint Commission and OSHA inspection in tracked deployments [3]. The evidence surveyors request already exists in the system. There’s no compilation step.
Technology doesn’t solve everything. When surveyors interview your night shift and hear that staff don’t activate the system because they believe nothing will change, your documented response times don’t matter. The technology produces records. The culture determines whether those records reflect reality.
The Comparison
This matrix maps documentation and technology evidence against the specific criteria surveyors use during accreditation visits.
Surveyor Criterion
Documentation Evidence
Technology Evidence
The Question to Ask
Response time capability
Estimated from incident reports, reconstructed after the fact
Timestamped from alert initiation through responder arrival
Can you produce response timestamps within 30 minutes of a surveyor request?
Coverage verification
Self-reported coverage maps from periodic walkthroughs
Manual reporting dependent on staff willingness and awareness
Automated capture with location, timestamp, and response data
What percentage of incidents actually reach your system?
Continuous monitoring proof
Periodic audits and spot checks with no continuous verification
System availability records showing consistent operation over 90+ days
Can you prove your safety system was operational every day for the past quarter?
Trending data availability
Compiled after survey announcement, may lack unit-level detail
Rolling 90-day data analyzed by unit, shift, and time period
Do you have 90 days of trending data ready to produce today?
Staff readiness evidence
Training attendance records with annual sign-offs
Staff preparedness metrics showing measurable improvement over time [3]
Can your staff demonstrate competency, or just prove they attended?
The pattern across facilities: documentation evidence establishes that a program exists. Technology evidence proves it works. Surveyors can tell the difference within minutes of reviewing your records.
Before your next survey window, assess where your current evidence falls on the comparison matrix:
Response time test. Request your own 90-day response data. Can your team produce it in under 30 minutes? If it requires manual compilation from multiple systems, you’re in the documentation column.
Coverage walkthrough. Walk your stairwells, parking structures, and outdoor areas. Can staff activate duress from every location, or are there dead zones you’ve been assuming don’t exist?
Incident capture reality check. Compare your incident logs to what your night-shift nurses would describe in a confidential surveyor interview. If those numbers don’t align, your records aren’t capturing reality.
Trending data readiness. Do you have 90 days of incident data analyzed by unit, shift, and time period ready to produce today? Not after a week of compilation. Today.
Staff competency verification. Pull three staff from different shifts this week. Ask them to describe the response protocol in their own words. Note who hesitates.
The staff duress deployment comparison between documentation and technology evidence comes down to one question: can you show a surveyor that your program produces outcomes, or only that it exists? For CMOs preparing for accreditation, the evidence portfolio you build determines which answer your organization gives.
EVIDENCE COMPARISON
See What Technology Evidence Looks Like at Your Facility
Behavioral health facilities with documented safety systems produce the evidence surveyors request on demand. See how documentation and technology evidence compare for your organization.
Surveyors verify staff awareness through targeted interviews, and your medical staff’s answers determine whether your violence prevention program passes or fails.
The CMO’s role isn’t to prepare every team directly but to coordinate across departments so clinical staff, physicians, and APPs can all demonstrate competency on demand.
Documentation that shows active capability, not just policy existence, is what separates a confident survey from a citation.
When a surveyor turns to one of your physicians and asks them to describe your facility’s violence prevention protocols, what happens next depends on what you’ve built. Not the policy binder. Not the training sign-in sheet. Whether your medical staff can walk through the protocols in their own words, explain the alert system, and describe de-escalation techniques they’ve actually practiced. That’s the clinical safety program evidence surveyors evaluate, and preparing your clinical teams to deliver it is the CMO’s job.
What Surveyors Ask Your Clinical Staff
The 2024 Joint Commission standards require surveyors to verify staff awareness through direct interviews. They ask staff to: [1]
Describe what counts as workplace violence in their facility
Explain the alert protocol or emergency response procedure
Walk through de-escalation techniques they’ve been trained on
Explain how to report a violent incident
Your medical staff need to answer these confidently. Distributing policies isn’t enough. Staff need to articulate protocols in their own words and show they understand how to apply them.
Here’s what typically happens across behavioral health facilities: staff can recite policy language but stumble on specifics. “What do you do if a patient in the day room becomes aggressive toward another patient?” The answer shouldn’t require checking a laminated card.
In facilities with documented safety systems, staff who feel “very prepared” to respond to incidents nearly doubled after deployment. [2] Those gains require sustained reinforcement though. Without quarterly refreshers, preparedness scores tend to drift back toward baseline.
Preparation plans for nursing staff on the four surveyor questions
30 days before survey window
CMO (you)
Physician and APP competency verification, including attendings and locum tenens
30 days before survey window
Unit Managers
Rapid competency checks with sample staff from each unit
14 days before survey window
HR/Education
Locum tenens and new attending orientation with documented competency
Ongoing
Physicians are the gap most CMOs miss. Your attendings may know clinical protocols cold but can’t describe the duress alert sequence. APPs rotate across units and may not know facility-specific response procedures. Locum tenens are the highest risk. Surveyors may interview anyone, and a locum who started last week gets the same questions as a 10-year veteran.
If your survey window opens in less than 3 months and you have high physician turnover, prioritize locum tenens and new attendings first. The four questions above are the prep list.
Documentation Surveyors Request
Surveyors want specific evidence your program works, not just that it exists. They request response time data, system reliability records, incident investigation trails, and governance reporting. [3]
Surveyor Request
What They Want
Your Production Window
Response time trending
Alert-to-arrival timestamps by unit, shift, and incident type
Within 30 minutes
System reliability
Uptime records and coverage verification
Within 30 minutes
Incident investigation
Each incident with timeline, investigation notes, and resolution
Facilities with documented response times show 93% of incidents resolved in under 2 minutes. [2] That’s the kind of benchmark your quality committee can report to governance. Think of it like a flight recorder for every incident. You can’t argue with timestamps.
Work with your CSO to verify response time tracking exists. Make sure your compliance officer can pull incident investigation records. Your role as CMO is confirming these systems produce the evidence surveyors request within the timeframes above.
Joint Commission has issued over 100 requirements for improvement related to workplace violence since January 2022. [1] Governance reporting receives particularly high scrutiny. Surveyors check whether your quality committee minutes show actual discussion of violence prevention trends, not just slides presented.
If your survey window is approaching and you need help coordinating clinical team readiness, we can walk you through it.
Facilities with documented safety technology show 39% reduction in patient-staff incidents in the first 3 months. [2] Worth noting: if your current incident capture is incomplete, numbers may actually increase early on as you capture events that previously went undocumented. That’s not failure. That’s visibility.
Pre-survey checklist:
Pull your last 3 quality committee minutes. Do they show documented discussion of violence prevention trends, or just slides?
Select 5 staff members randomly across units. Can each answer the four surveyor questions without prompting?
Request response time data for the past 90 days. Can your system produce it within 30 minutes?
Review post-incident records for the past quarter. Is follow-up documented for each event?
For enterprise behavioral health organizations, consistency across facilities matters. Corporate sets standards, facilities execute. Surveyors may visit any site, and inconsistency across locations is a common citation area.
Start with one question: can your medical staff articulate your clinical safety program protocols when a surveyor asks? If the answer is “I’m not sure,” that’s your first gap to close.
SURVEY READINESS
Prepare Your Clinical Teams with Documented Evidence
Facilities with documented safety systems show 93% of incidents resolved in under 2 minutes. See what survey-ready evidence looks like for your clinical program.
Surveyors evaluate violence prevention by looking for proof of action, not policy binders, across four categories: staff awareness, response capability, incident tracking, and leadership accountability.
Organizations that generate continuous records pass surveys confidently because they can hand over the exact evidence surveyors request on demand.
The gap between having a program and proving it works is where most accreditation failures start, and closing that gap means building systems that document what happens automatically.
Accreditation surveys expose a gap most behavioral health leaders don’t see coming. Your violence prevention program may be thorough. Your staff may be well-trained. Your protocols may work. But if you can’t hand a surveyor documented proof of all three, none of it counts. Staff duress deployment that generates continuous evidence is what separates a confident walkthrough from a scramble, and surveyors can tell the difference in minutes.
What Joint Commission Surveyors Actually Evaluate
The 2024 Joint Commission standards for behavioral health changed what surveyors look for. Three new requirements and one revised standard now demand proof that programs are working, not just that they exist. Surveyors check whether each requirement is met, partially met, or not met based on what you can show them. [1]
Behavioral health settings face the highest workplace violence rates in healthcare. Psychiatric and substance abuse hospitals see roughly 11 times the rate of incidents compared to the general workforce. [2] Surveyors know this. They arrive expecting programs that match the reality staff face every shift.
What they want to see: that violence prevention policies exist and are practiced, that incident reporting and trend analysis actually function, that follow-up support for affected staff is documented, and that incidents reach leadership. [3]
The key phrase is “put into practice.” Surveyors don’t just read your policies. They watch, they interview staff, and they review records. They’ll pull a random incident from months ago and trace every step of the response. If the records stop at the initial report, they notice. [4]
“Surveyors don’t just read your policies. They watch, they interview staff, and they review records. They’ll pull a random incident from months ago and trace every step of the response.”
That’s the challenge. Your program might be effective. But if you can’t produce the documentation, surveyors can’t verify it.
Want to understand what this looks like at your facility? Talk to us.
The Four Evidence Categories Surveyors Require
Surveyors look at violence prevention across four categories. Knowing what they request in each one shows why passing is harder than it looks.
Staff Awareness
Healthcare settings must train staff at hire, annually, and whenever changes happen. Surveyors check whether training covers what counts as workplace violence, who does what during a response, de-escalation skills, emergency procedures, and how to report incidents. [5]
Here’s where teams get stuck. Sign-in sheets prove attendance. Surveyors want proof of competency. They want to know that training covered de-escalation specific to your patient population and that staff actually retained it. Facilities with documented preparedness data can show measurable improvement in how confident staff feel responding to incidents. [6] Without that, training compliance is just a claim.
Response Capability
Surveyors want to know your team can respond when something happens. They check whether response systems actually work, stay reliable, and leave a paper trail.
When a surveyor asks “how quickly does help arrive when staff press the button,” they expect real data. Facilities with documented response times can answer precisely: in tracked deployments, more than 9 in 10 incidents resolve in under two minutes. [6] “We think it’s usually pretty fast” doesn’t cut it.
System reliability matters too. Surveyors check whether your safety systems stay available consistently. They also test coverage. They’ll walk to the loading dock, the basement, the stairwell between floors and ask staff to show duress activation. Systems with facility-wide coverage eliminate the dead zones that make those moments uncomfortable. [6]
Incident Tracking
Psychiatric units need continuous monitoring, internal reporting, and investigation processes for safety incidents. Surveyors want data that identifies the highest-risk locations, the times and types of incidents, and the conditions that contributed. They check whether your team uses that data to shape prevention. [4]
Fewer than 1 in 3 nurses say their employer gives them a clear way to report incidents. [7] Surveyors know this pattern. They know manual logs undercount what actually happens. When they review your data, they’re judging not just what you documented but whether your system captures reality.
The follow-through matters as much as the initial report. Surveyors pull sample incidents and trace the investigation: root cause analysis, corrective actions, follow-up interviews. When the trail goes cold after the first report, that’s a failed element. Joint Commission data shows leadership failure in follow-through as a factor in nearly 2 in 3 violent incident events. [8] The committee exists. The policy says investigate. But the documented follow-up stops at the initial report.
Leadership Accountability
Surveyors check whether violence prevention has designated leadership and multidisciplinary oversight. They want proof that incidents reach governance and that leadership is actively engaged with outcomes. Deficiencies here come from inadequate oversight of action, not from missing programs. [8]
Evidence Category
What Surveyors Request
Common Gap
Staff Awareness
Training completion with competency proof
Sign-in sheets without content verification
Response Capability
Response time data and system reliability
Anecdotal estimates without measurement
Incident Tracking
Trending analysis and investigation records
Initial reports without follow-up
Leadership Accountability
Governance reporting and active oversight
Committee existence without documented activity
Where Facilities Actually Fail
Facilities don’t fail surveys because they lack policies. They fail because they can’t show action.
The Underreporting Problem
More than 8 in 10 workplace violence incidents go unreported by the workers who experienced them. [9] Surveyors know this. When they look at your incident logs, they’re asking whether your numbers reflect what actually happens or just a fraction of it.
Nearly 9 in 10 workers don’t formally document incidents in their facility’s central database. [10] The reasons are consistent: staff believe reporting won’t change anything, they see violence as “part of the job,” and the reporting process itself is too cumbersome. Surveyors treat underreporting as a sign that the safety culture isn’t working.
That creates a paradox. Hospitals with more documented incidents may actually show stronger compliance than hospitals with fewer. Surveyors aren’t looking for low numbers. They’re looking for evidence your system captures what really happens.
“Hospitals with more documented incidents may actually show stronger compliance than hospitals with fewer. Surveyors aren’t looking for low numbers. They’re looking for evidence your system captures what really happens.”
The Investigation Problem
Reporting alone isn’t enough. Surveyors check that reported incidents get real follow-up. Your team has to show they “report and investigate.” [4]
OSHA and Joint Commission enforcement cases show a consistent pattern of deficiencies: records limited to incidents that needed first aid rather than all incidents, weak review processes, outdated policies no one communicated, and no organized follow-up on staff safety suggestions. [11]
Nearly half of nurses say workplace violence incidents are simply ignored after being reported. [7] Surveyors test this by reviewing actual records and asking staff directly how investigations work. Paper processes without documented execution don’t hold up.
What Failure Costs
When facilities show serious noncompliance, Joint Commission can issue Preliminary Denial of Accreditation. That triggers follow-up reviews and can suspend the designation that lets you bill Medicare and Medicaid. [12]
The financial exposure is real: losing accreditation can put millions in annual funding at risk. [13] Beyond money, it threatens clinical programs, physician recruitment, and the care environment you’ve spent years building.
Deficiency Pattern
Root Cause
How Surveyors Find It
Incomplete incident records
Manual reporting barriers
Reviewing logs for gaps
Missing investigation follow-up
No systematic process
Tracing sample incidents
Unverified training competency
Sign-in sheets only
Interviewing staff about content
Undocumented response capability
No measurement system
Direct observation and timing
If your team is preparing for an upcoming survey, we can walk you through what documentation surveyors typically request.
Behavioral health facilities with documented safety technology show a clear advantage during surveys. Automated systems create continuous records of incident reporting, training completion, and response data. That’s exactly what Joint Commission requires when it asks for ongoing monitoring and trending. [4]
What Automated Records Actually Produce
Staff duress deployment with automated records generates the specific evidence surveyors ask for:
Staff Awareness: Training completion with competency proof. Preparedness data showing measurable improvement over time.
Response Capability: Response time tracking with historical trends. Reliability records. Coverage verification with no dead zones.
Incident Tracking: Timestamped records with location data. Automated trending by unit, shift, and acuity level. Investigation workflow documentation.
Leadership Accountability: Exportable audit logs for governance reporting. Dashboard visibility into program metrics. Continuous monitoring evidence.
Behavioral health facilities using documented staff duress deployment have passed every Joint Commission and OSHA inspection in tracked deployments. [6] When surveyors ask for evidence, these facilities hand it over immediately.
The advantage comes from generating evidence continuously rather than scrambling before audits. Manual systems have gaps, inconsistent reporting, and trouble identifying trends. Automated systems create the verifiable audit trails surveyors specifically look for. [4]
Surveyor Request
Manual Response
Automated Response
“Show me response time trending”
Estimates or no data
Dashboard with historical records
“How do you track incidents by location?”
Spreadsheet requiring manual work
Real-time visualization by unit
“What’s your system uptime?”
Unknown or estimated
Documented reliability records
“Can staff show the duress protocol?”
Depends on training
Consistent with documented competency
Beyond passing surveys, facilities show roughly 40% reduction in violent incidents within the first year. [6] The same records that satisfy surveyors drive real quality improvement.
Preparing for Survey Success
Joint Commission expects continuous readiness, not last-minute preparation. Best practice means conducting mock surveys at least six months before your triennial date and running internal compliance checks quarterly. [14]
Mock Survey Priorities
Mock surveys should cover the same ground real surveyors cover:
Staff interviews about duress response protocols and training content
Direct observation of system activation and response timing
Review of incident records for investigation follow-up
Assessment of trending data availability
Verification of governance reporting processes
The Quick Readiness Check
Four questions that cut through the noise:
Can you export 90 days of incidents by unit in one click? If it takes 20 minutes and a spreadsheet, that’s a problem.
Can you find proof leadership reviewed trends monthly? Not slides. Minutes with actual discussion.
Grab two random staff from different units and ask: “What happens if de-escalation fails?” If they hesitate, your training records don’t matter.
Does response time data exist, or are you guessing?
Continuous Over Episodic
The strongest facilities maintain safety culture year-round. Quality improvement research shows meaningful reduction in violence incidents when continuous approaches run for 15 months or longer. [15] The goal isn’t to pass the next survey. It’s to build systems that make survey prep unnecessary because the evidence generates itself.
No one should face violence while trying to help others heal. Your staff duress deployment should deliver on that standard, and your records should prove it.
ACCREDITATION READINESS
Build Survey Confidence with Documented Evidence
Facilities using staff duress deployment with automated records have passed every Joint Commission and OSHA inspection in tracked deployments. See what continuous compliance looks like.
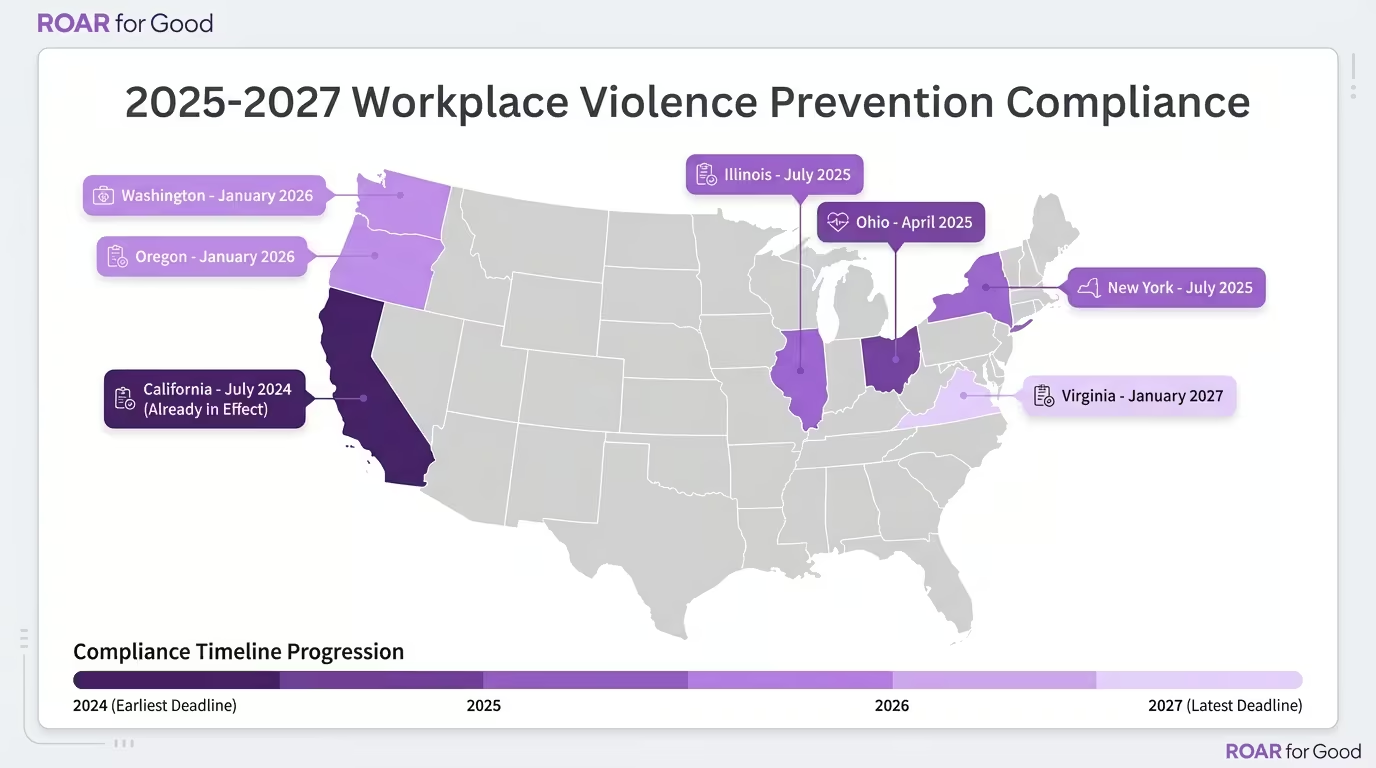
State workplace violence laws have shifted from advisory guidelines to enforceable mandates with real deadlines—Ohio’s requirements took effect April 2025, Illinois demands panic buttons by July, and nine more deadlines land before 2027.
Building infrastructure to meet the strictest standard (Illinois SB1435) automatically satisfies less prescriptive requirements in Ohio, California, Washington, and beyond—one investment covers the patchwork.
Getting ahead of the compliance wave protects your facilities from compounding penalties while positioning your system as a safety leader that attracts and retains staff.
The 2025 Enforcement Wave: What Changed
Until 2024, most state workplace violence laws were advisory or lacked enforcement teeth. That’s over.
Ohio became the first state to sign comprehensive hospital violence prevention into law on January 8, 2025, following a nurse’s death in Dayton [6]. Illinois followed with the nation’s first panic button mandate for hospital employees [2]. Washington enhanced its existing framework with annual plan reviews and detailed incident reporting [3].
The shift: requirements now come with deadlines, reporting obligations, and—in some cases—direct penalties for non-compliance.
2025-2027 Compliance Calendar
Deadline
State
Law
Key Requirements
April 9, 2025
Ohio
HB 452
Security plans, incident reporting, de-escalation training in ED/psych, employee input required [1]
July 1, 2025
Illinois
SB 1435
Panic buttons attached to staff ID cards for all hospital employees [2]
July 1, 2024
California
SB 553
WVPP for all employers, incident logs (5-year retention), annual training [7]
July 1, 2025
New York
A203
Violence prevention programs; security personnel in high-volume EDs [8]
January 1, 2026
Washington
HB 1162
Annual plan reviews, enhanced incident data reporting, safety committee oversight [3]
January 1, 2026
Oregon
HB 2552
Safety committees, incident data reporting to state, grant program for prevention [9]
January 1, 2027
Virginia
HB 1919
WVPP required for employers with 100+ employees [9]
TBD 2025-2026
Federal
OSHA Standard
Proposed rule for healthcare; comment period expected [10]
Pending
Federal
H.R.2531
Workplace Violence Prevention for Healthcare Workers Act—would mandate OSHA standard [5]
MULTI-STATE SYSTEMS
One investment. Every state covered.
OSHA fined a Florida healthcare company $100K+ in 2024—before any formal standard existed. Know where you stand.
OSHA fined a Florida healthcare company over $100,000 in May 2024 for violence prevention failures—using the General Duty Clause before any formal standard existed [10].
Illinois Sets the Standard: What Panic Button Mandates Mean
Illinois SB1435 is the first state law to explicitly require wearable panic buttons for hospital employees [2]. The bill amends both the University of Illinois Hospital Act and Hospital Licensing Act, requiring that all employees have a panic button attached to their staff identification card by July 1, 2025.
Why this matters for multi-state systems: Infrastructure deployed to meet Illinois requirements—wearable devices with location tracking and instant alerting—will satisfy the less prescriptive “prevention plan” requirements in Ohio, California, Washington, and other states. Building to the highest standard eliminates re-work as other states follow Illinois’s lead.
MULTI-STATE SYSTEMS
One investment. Every state covered.
OSHA fined a Florida healthcare company $100K+ in 2024—before any formal standard existed. Know where you stand.
The common thread across state requirements: rapid response, facility-wide coverage, and documented incident tracking.
Requirement Category
States Requiring
Infrastructure Solution
Written prevention plan
CA, OH, WA, TX, NY, VA
Plan development + technology documentation
Incident reporting/logs
CA, OH, WA, OR
Automated logging with 5-year retention
Employee training
All Tier 1 & 2 states
Integrated onboarding + annual refreshers
De-escalation personnel
OH (ED/psych), NY (high-volume ED)
Trained staff + alert routing to responders
Panic buttons/alert devices
IL (explicit mandate)
Wearable BLE devices with room-level accuracy
Safety committees with employee input
OH, WA, OR, PA (pending)
Committee reporting + analytics dashboards
Systems that deploy network-independent alert technology—operating without Wi-Fi or cellular dependency—satisfy the reliability requirements implied across all state frameworks while eliminating coverage gaps that create liability exposure.
Operating across multiple states? Contact us to map your compliance exposure and identify which requirements your current infrastructure already satisfies.