Key Takeaways
- Most cost estimates boards review reflect a fraction of actual incidents, meaning the real financial exposure from workplace violence is far larger than anyone in the room assumes.
- Peer behavioral health organizations have documented 40% assault reductions within six months of deploying structured safety technology.
- You can build a solid financial model using inputs from your own facility: current workers’ comp claims, annual nursing turnover, and open position count.
Your board wants staff duress solution data. Your CNO has made the safety case. Your CFO wants sourced numbers. But when a skeptical director asks what comparable behavioral health organizations have actually measured, most CEOs can’t produce a consolidated evidence brief.
What Inaction Costs Behavioral Health Organizations
Workplace violence costs U.S. hospitals $18.27 billion annually [1]. That figure includes $13.1 billion in treatment for violent injuries and $584 million in infrastructure repairs.
For behavioral health, the exposure is worse. Psychiatric aides experience a workplace injury rate of 543.6 per 10,000 workers, the highest in the Bureau of Labor Statistics dataset [2].
The number that changes the conversation: 81% of workplace violence incidents go unreported [3]. Your board is making decisions based on the visible portion of the problem. The financial exposure underneath is roughly four times larger than what anyone in the room can document.
When incidents do surface, the penalties stack. OSHA maximum fines for willful violations reach $165,514 per violation in 2025 [4].
Staff Duress Solution Data: Documented Outcomes Across Peer Facilities
Peer behavioral health organizations have documented enough outcomes to move past anecdotes. The strongest results, with methodology context a skeptic can evaluate:
| Organization Type | Metric | Result | Timeline | Methodology |
|---|---|---|---|---|
| National behavioral health provider | Assaults against staff | 40% reduction | 6 months | ROAR customer data, pre/post measurement [5] |
| Behavioral health center (BeWell) | Workers’ comp claims | 24% decrease | Post-deployment | ROAR customer data, pre/post measurement [5] |
| National behavioral health provider | Workers’ comp claims | 50% decrease | Post-deployment | ROAR customer data, pre/post measurement [5] |
| Hospital intervention units (RCT) | Violent incident rates | 52% lower vs. controls | 6 months | Peer-reviewed RCT (non-U.S.; comprehensive program, not technology alone) [6] |
A note on methodology: customer outcomes are pre/post measurements at individual facilities. The peer-reviewed finding used a randomized controlled design with a comprehensive intervention program. Concurrent interventions like training or staffing changes may contribute to outcomes at any facility. This transparency matters. A CFO who spots the distinction will trust the compilation more because of it.
Building the Financial Case Without Guesswork
The financial model requires no vendor calculator. Three cost-avoidance categories give your CFO something to stress-test with your own numbers:
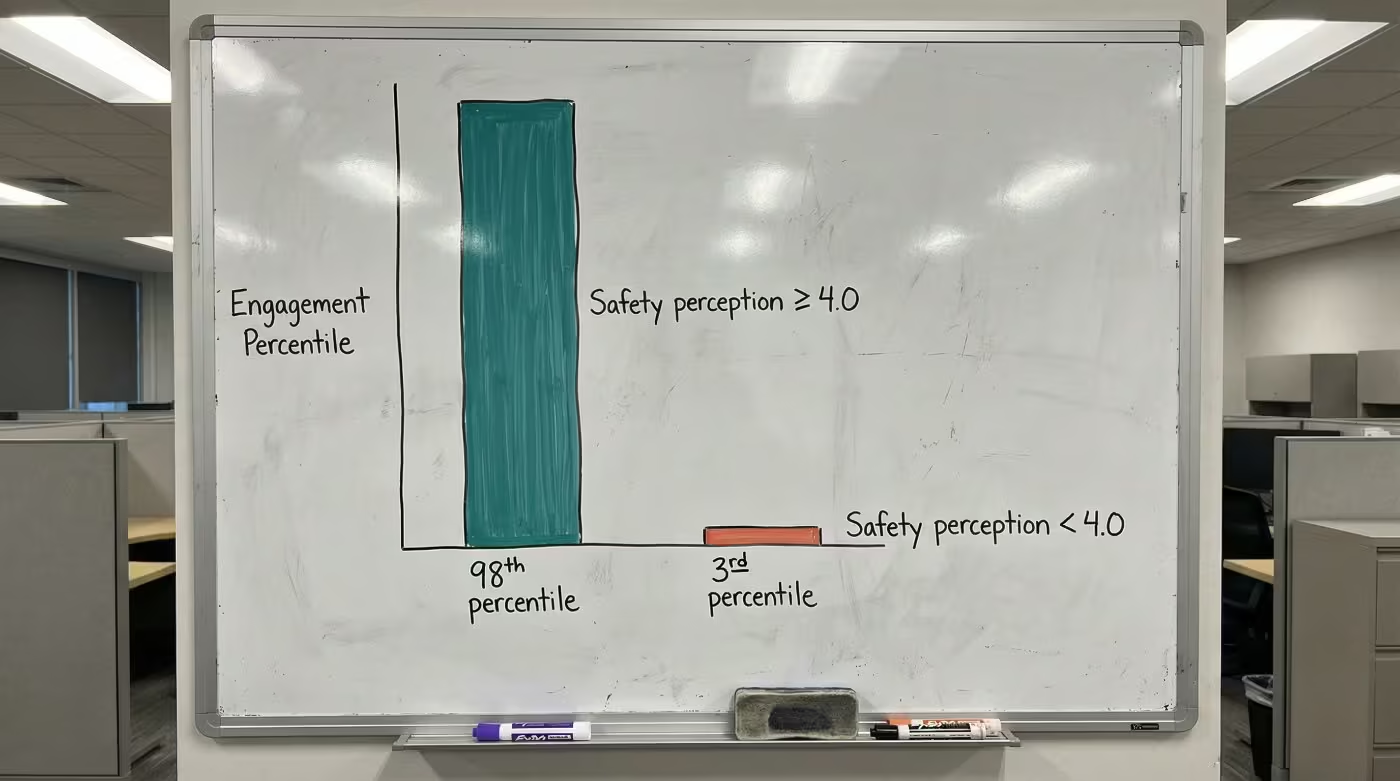
- Turnover cost avoidance. Replacing one bedside RN costs $61,110 [7]. At one customer facility, staff who said they’d consider leaving due to safety concerns dropped from 22% to 7% [5]. Apply that shift to your own headcount and replacement costs. Each percentage point of nursing turnover change saves or costs the average hospital $289,000 per year [8].
- Workers’ comp reduction. Use your facility’s average annual claims count. Apply the 24% to 50% reduction range documented above. Multiply by your average cost per claim.
- Vacancy cost avoidance. Industry analysis estimates each vacant behavioral health clinician position generates roughly $30,000 in unbillable appointment costs per quarter [9]. Count your current open positions.
These ranges reflect outcomes at specific peer facilities; your results will depend on your current claims volume, turnover rate, and baseline incident frequency.
The model is yours to adapt. Plug in your numbers, share the inputs with your CFO, and let them challenge the assumptions.
See how one behavioral health provider documented these results across their facilities.
Effort Versus Return in Real Deployments
U.S. hospitals spend $1.4 billion annually on violence prevention training [1]. The question is whether that spend produces measurable outcomes.
| Approach | Staff Hours Required | Timeline to Results | Documented Outcome |
|---|---|---|---|
| De-escalation training (150 staff) | 1,200 to 2,400 hours (estimates vary by program) | Varies | Varies by program |
| Technology deployment (duress system) | Minimal staff hours; no disruption to patient care reported | Under 6 months to measurable value [5] | 40% assault reduction; up to 50% workers’ comp decrease [5] |
Behind every data point is a staff member who went home safer. That’s what rapid response time means in practice: the gap between pressing a button and getting help nearly disappears.
These gaps are common. Most organizations start here. Peer organizations that built their case from evidence like this found the board conversation went better than expected.
A behavioral health safety specialist can walk you through how these numbers apply to facilities like yours.
Contact UsYour Board-Ready Evidence Summary
This summary lifts directly into a board memo or executive briefing.
| Category | Key Finding | Source | Methodology Note |
|---|---|---|---|
| Cost of inaction | $18.27B annual cost to U.S. hospitals; 81% of incidents unreported | AHA 2025; AHRQ | Industry-wide estimates; underreporting inflates true exposure |
| Peer outcomes | 40% assault reduction in 6 months; 24% to 50% workers’ comp decrease | ROAR customer data | Pre/post measurement at customer facilities |
| Financial model inputs | $61,110 per RN replacement; $289,000 per 1% turnover change | Plexsum 2025; NSI 2025 | Published industry benchmarks |
| Regulatory compliance | 100% Joint Commission and OSHA inspection pass rate post-deployment | ROAR customer data [5] | Facilities with automated duress systems |
Board members typically ask three questions:
- Where did these numbers come from? Every figure above includes its source.
- Could something else explain the improvement? The methodology notes flag where concurrent factors may contribute.
- What’s the timeline? Peer outcomes were measured within six months.
This evidence brief on staff duress solution data is built to be reused. Save it. Return to it before your next board meeting, your next CFO conversation, your next budget cycle. The data points are sourced, the methodology context is included, and the financial model is yours to adapt.
PEER EVIDENCE
Ready to Build Your Evidence Brief?
See the documented outcomes from behavioral health organizations comparable to yours.
References
- American Hospital Association. (2025). New AHA Report Finds Workplace and Community Violence Cost Hospitals More Than $18 Billion. https://www.aha.org/press-releases/2025-06-02-new-aha-report-finds-workplace-and-community-violence-cost-hospitals-more-18-billi
- Bureau of Labor Statistics. (2025). Workplace Violence 2021-2022 Fact Sheet. https://www.bls.gov/iif/factsheets/workplace-violence-2021-2022.htm
- Agency for Healthcare Research and Quality. Addressing Workplace Violence and Creating a Safer Workplace. https://psnet.ahrq.gov/perspective/addressing-workplace-violence-and-creating-safer-workplace
- Safety+Health Magazine. (2025). OSHA and MSHA Civil Penalty Amounts Going Up. https://www.safetyandhealthmagazine.com/articles/26317-osha-and-msha-civil-penalty-amounts-going-up
- ROAR for Good. Internal Data, 2024.
- National Center for Biotechnology Information. Hospital Violence Prevention Intervention Study. https://pmc.ncbi.nlm.nih.gov/articles/PMC5214512/
- Plexsum. (2025). The Real Cost of Nurse Turnover: What Hospitals Need to Know in 2025. https://plexsum.com/2025/04/08/the-real-cost-of-nurse-turnover-what-hospitals-need-to-know-in-2025/
- NSI Nursing Solutions. (2025). National Health Care Retention Report. https://www.nsinursingsolutions.com/documents/library/nsi_national_health_care_retention_report.pdf
- Continuum Cloud. True Cost of Turnover in Behavioral Health. https://continuumcloud.com/blogs/true-cost-of-turnover-in-behavioral-health-how-hr-leaders-can-reduce-it/